
Peripheral neuropathy is a common and often debilitating condition that affects millions of people worldwide. Chronic pain, numbness, tingling, and muscle weakness significantly reduce quality of life, especially when standard treatments fail to provide relief. In recent years, stem cell therapy for neuropathy has gained attention as a potential regenerative and anti-inflammatory approach. But how effective is it, and what should patients realistically expect?
OBSERVE NEW : STEM CELLS PROTOCOL OF NEUROPATHY THERAPY 2026
What Is Neuropathy?
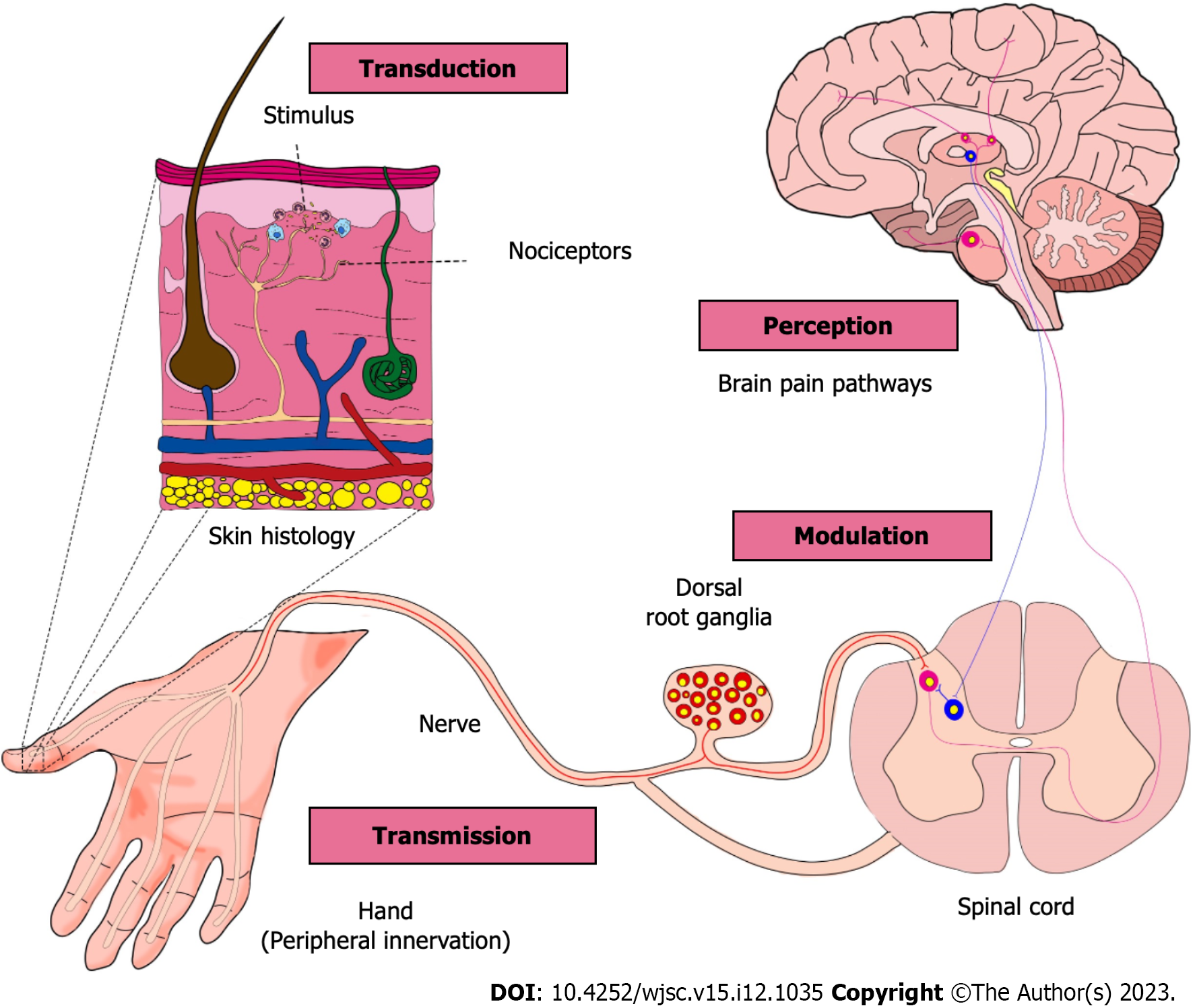
Neuropathy refers to damage or dysfunction of peripheral nerves that transmit signals between the brain, spinal cord, and the rest of the body. It can affect sensory, motor, or autonomic nerves.
Common causes of neuropathy include:
- Diabetes (diabetic neuropathy)
- Autoimmune diseases
- Chemotherapy-induced nerve damage
- Vitamin deficiencies
- Chronic inflammation
- Trauma or nerve compression
- Idiopathic neuropathy (unknown cause)
Conventional treatment usually focuses on symptom management, not nerve repair.
Why Patients Consider Stem Cell Therapy for Neuropathy
Many patients search for stem cell treatment after experiencing:
- Persistent nerve pain despite medication
- Progressive numbness or loss of sensation
- Side effects from long-term drug use
- Limited improvement with physical therapy
Stem cell therapy is being explored because it aims to support nerve healing rather than only masking symptoms. Learn more about stem cells treatment of neuropathy: Can stem cells therapy help with polyneuropathy in 2025?
How Stem Cell Therapy May Help Neuropathy
Current research suggests that stem cells may support nerve recovery through several biological mechanisms:
1. Anti-inflammatory Effects
Chronic inflammation plays a major role in nerve damage. Mesenchymal stem cells (MSCs) can modulate immune responses and reduce inflammatory signaling around affected nerves.
2. Neuroprotection
Stem cells release bioactive molecules that may help protect existing nerve fibers from further degeneration.
3. Paracrine Signaling
Rather than replacing nerves directly, stem cells secrete growth factors and cytokines that:
- Support nerve regeneration
- Improve microcirculation
- Enhance local tissue repair
4. Support of Schwann Cells
Schwann cells are essential for nerve repair and myelin regeneration. Stem cell signaling may indirectly stimulate their activity.
Importantly, stem cell therapy is not considered a cure for neuropathy, but a potential regenerative support strategy.
What Does the Research Say?
Clinical studies and early-phase trials suggest that stem cell therapy may improve pain, sensation, and nerve conduction in some patients with neuropathy, particularly diabetic and inflammatory forms.
However:
- Results vary significantly
- Large-scale randomized trials are still limited
- Long-term outcomes are still being evaluated
This is why most reputable clinics present stem cell therapy as experimental or adjunctive, not as a guaranteed solution.
Diabetic Neuropathy
Diabetic neuropathy is the most common form of peripheral neuropathy and is primarily caused by chronic hyperglycemia, microvascular damage, and persistent low-grade inflammation. In these cases, research and clinical protocols most often focus on mesenchymal stem cells (MSCs) due to their strong anti-inflammatory, angiogenic, and neuroprotective properties. MSCs may help improve microcirculation, reduce oxidative stress, and support nerve fiber survival. In some advanced protocols, endothelial progenitor cells (EPCs) are also explored to address vascular insufficiency, which is a key factor in diabetic nerve damage.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
Chemotherapy-induced neuropathy results from direct neurotoxic effects on sensory neurons and supporting glial cells. In this context, treatment strategies typically emphasize neuroprotective and paracrine mechanisms rather than direct nerve replacement. Mesenchymal stem cells are again the primary cell type used, particularly for their ability to secrete neurotrophic factors that may support damaged sensory neurons. Some approaches also investigate neural progenitor cell–derived secretomes or MSC-derived exosomes to reduce neuroinflammation without introducing highly proliferative cells.
Autoimmune-Related Neuropathy
Neuropathy associated with autoimmune diseases such as rheumatoid arthritis, lupus, or chronic inflammatory demyelinating polyneuropathy (CIDP) is driven largely by immune-mediated nerve injury. In these cases, immunomodulatory cell populations are of particular interest. Mesenchymal stem cells are favored because of their capacity to downregulate aberrant immune responses and promote immune tolerance. Some research protocols also explore regulatory immune-supportive cell fractions, aiming to reduce ongoing immune attack on peripheral nerves rather than focusing solely on regeneration.
Idiopathic Neuropathy
Idiopathic neuropathy is diagnosed when no clear underlying cause can be identified, despite thorough evaluation. Because the pathological mechanism is often multifactorial, treatment approaches tend to be broader. Mesenchymal stem cells are commonly selected for their wide-ranging paracrine effects, including anti-inflammatory signaling, support of Schwann cell activity, and enhancement of local tissue repair. In idiopathic cases, therapy is generally considered supportive, with the goal of symptom reduction and stabilization rather than targeted correction of a single pathway.
Traumatic and Compression-Related Neuropathy
Neuropathy caused by trauma, surgical injury, or chronic nerve compression involves localized nerve damage and impaired regeneration. In these scenarios, regenerative strategies may include MSCs combined with Schwann cell–supportive signaling, as Schwann cells play a central role in peripheral nerve repair and remyelination. Some experimental studies investigate Schwann cell–like differentiated MSCs, designed to enhance axonal guidance and myelin restoration, although these approaches remain largely investigational.
Small Fiber Neuropathy
Small fiber neuropathy predominantly affects thin, unmyelinated sensory fibers responsible for pain and temperature sensation. Because these fibers are highly sensitive to inflammatory and metabolic disturbances, treatment strategies often focus on anti-inflammatory and neurotrophic support. Mesenchymal stem cells are again the most commonly explored option, particularly for their ability to release nerve growth factors and reduce neuroinflammation. Direct replacement of small sensory fibers is not currently feasible, making paracrine-based approaches the primary focus.
OUR CLINICAL PROTOCOL OF USING NARROW DIFFERENTIATED STEM CELL IN NEUROPATHY TREATMENT
Neural Stem Cells in Neuropathy Treatment
Neural stem cells (NSCs) are being investigated for their potential role in supporting nerve repair in selected neuropathic conditions. Unlike mesenchymal stem cells, NSCs are lineage-committed cells capable of differentiating into neurons and glial cells. In experimental and early clinical research, neural stem cells are primarily explored in cases of severe or progressive neuropathy, where direct support of neural networks may be beneficial. Their proposed role is not full nerve replacement, but rather local neurotrophic support, modulation of the neural microenvironment, and interaction with existing nerve structures. Due to their specialized nature, the use of neural stem cells remains limited to controlled research settings.
Endothelial Progenitor Cells and Vascular-Related Neuropathy
Endothelial progenitor cells (EPCs) are of particular interest in neuropathies where microvascular dysfunction plays a central role, such as diabetic neuropathy or ischemic nerve injury. Nerve health is highly dependent on adequate blood supply, and damage to small vessels often precedes or exacerbates nerve degeneration. EPCs may contribute to angiogenesis, endothelial repair, and improved tissue perfusion, indirectly supporting nerve recovery. In regenerative protocols, endothelial cell–based approaches are sometimes considered complementary rather than standalone therapies, targeting the vascular component of neuropathy.
Combination Approaches: Stem Cells and Exosomes
Increasing attention is being given to cell-free or combination therapies involving stem cells and exosomes. Exosomes derived from mesenchymal or neural stem cells contain bioactive molecules such as microRNAs, growth factors, and signaling proteins that may mediate many of the therapeutic effects traditionally attributed to stem cells. In neuropathy research, exosomes are explored for their ability to reduce neuroinflammation, promote axonal support, and enhance Schwann cell activity. Combination strategies using stem cells together with their exosomes aim to amplify paracrine signaling while potentially reducing cellular risks.
Research more useful information: Peripheral neuropathy: How does stem cells therapy work?
Mitochondrial Support and Neuroregeneration
Mitochondrial dysfunction is increasingly recognized as a contributing factor in several forms of neuropathy, particularly metabolic and toxic neuropathies. Experimental approaches investigate whether mitochondrial transfer or mitochondrial-supportive vesicles derived from stem cells can help restore cellular energy balance in damaged neurons. While still largely preclinical, this strategy focuses on improving neuronal resilience and metabolic stability rather than structural nerve regeneration.
Anti-Inflammatory Cytokines and Immunomodulatory Molecules
Chronic inflammation is a key driver of nerve damage in many neuropathic conditions. Stem cell–based therapies are often valued for their ability to influence cytokine signaling rather than direct differentiation. Research protocols explore combinations of stem cells with anti-inflammatory cytokines, immunoregulatory vesicles, or secretome-based formulations to downregulate harmful immune activity around peripheral nerves. These approaches aim to create a more favorable environment for endogenous nerve repair.
A Multimodal Regenerative Strategy
Rather than relying on a single cell type or molecule, current research trends emphasize multimodal regenerative strategies. Combining stem cells, endothelial support, exosomes, and immunomodulatory factors reflects a growing understanding that neuropathy is a complex, multifactorial condition. Such combination approaches are designed to address inflammation, vascular impairment, metabolic dysfunction, and neural support simultaneously, while maintaining realistic expectations regarding outcomes.
Safety and Potential Risks
When performed under proper medical standards, stem cell therapy is generally considered well tolerated, but it is not risk-free.
Possible risks include:
Temporary pain or swelling at injection site
- Immune reactions (rare)
Patients should be cautious of clinics promising “complete nerve regeneration” or instant results.
Who May Be a Candidate for Stem Cell Therapy?
Stem cell therapy for neuropathy may be considered for patients who:
- Have chronic or progressive neuropathy
- Did not respond adequately to conventional treatment
- Have stable underlying conditions
- Do not have active infections or malignancies
Early-stage neuropathy often responds better than advanced nerve degeneration.
Treatment Process and Cost Considerations
While protocols vary, treatment often includes:
- Medical evaluation and diagnostics
- Cell preparation or harvesting
- Intravenous or localized administration
- Follow-up and monitoring
Costs differ widely depending on:
- Cell source and processing
- Number of sessions
- Country and regulatory environment
Stem cell therapy for neuropathy is typically not covered by insurance.

Clinical Outcomes Observed in Neuropathy Treatment
Clinical studies and observational reports suggest that stem cell–based approaches may lead to partial symptom improvement in selected patients with peripheral neuropathy. The most commonly reported benefits include reduction in neuropathic pain, decreased paresthesia, and improved sensory function. Improvements are typically described as moderate rather than complete, with outcomes depending on neuropathy type, disease duration, and underlying cause. Early-stage and inflammatory neuropathies tend to show more favorable responses compared to advanced axonal degeneration.
Pain Reduction and Functional Improvement
Across multiple small clinical studies and case series, pain reduction is one of the most consistently reported outcomes. Some reports describe measurable decreases in pain scores within weeks to months following treatment, particularly in diabetic and chemotherapy-induced neuropathy. Functional outcomes, such as improved balance, walking tolerance, or fine motor control, have also been noted, although these changes are often gradual and vary widely between individuals. Importantly, pain relief does not always correlate with objective nerve regeneration.
Sensory and Nerve Conduction Findings
Objective assessments such as nerve conduction studies and quantitative sensory testing have shown mixed results. In some cases, modest improvements in nerve conduction velocity or sensory thresholds have been observed, while in others no significant electrophysiological changes were detected despite subjective symptom relief. This discrepancy supports the hypothesis that paracrine and anti-inflammatory effects, rather than structural nerve replacement, account for many of the clinical benefits reported.
Clinical Case Observations
Published clinical case reports describe patients with long-standing neuropathy experiencing stabilization or partial symptom reversal following stem cell–based interventions. For example, some diabetic patients have reported reduced burning pain and improved foot sensation, while individuals with autoimmune-related neuropathy have shown decreased symptom fluctuation.
One of the most important findings across studies is the high variability in patient response. Factors associated with better outcomes include shorter disease duration, preserved nerve structure, controlled metabolic or autoimmune activity, and absence of severe fibrosis. Conversely, patients with advanced axonal loss or long-standing denervation often experience limited or no measurable benefit. These observations highlight the importance of patient selection and realistic expectations. Find more about benefits: Stem Cell Therapy – When to Expect Results
Follow-up data suggest that reported improvements may persist for 16 months and more , in some cases, longer periods. However, long-term durability remains insufficiently studied, and repeat or adjunctive treatments are sometimes explored in research settings. There is currently no consensus on optimal dosing, frequency, or maintenance strategies for stem cell–based neuropathy treatment.
Final Thoughts
Stem cell therapy for neuropathy represents a promising area of regenerative medicine, particularly for patients with limited treatment options. While early results are encouraging, it is essential to approach therapy with realistic expectations, thorough medical evaluation, and evidence-based decision-making.
Patients considering this option should seek qualified medical professionals, transparent protocols, and clear communication about potential benefits and limitations.
GET FREE ONLINE CONSULTATION
