Why We Select Specific Cellular Cultures
A personalized ALS protocol often includes carefully selected cellular types based on therapeutic goals.
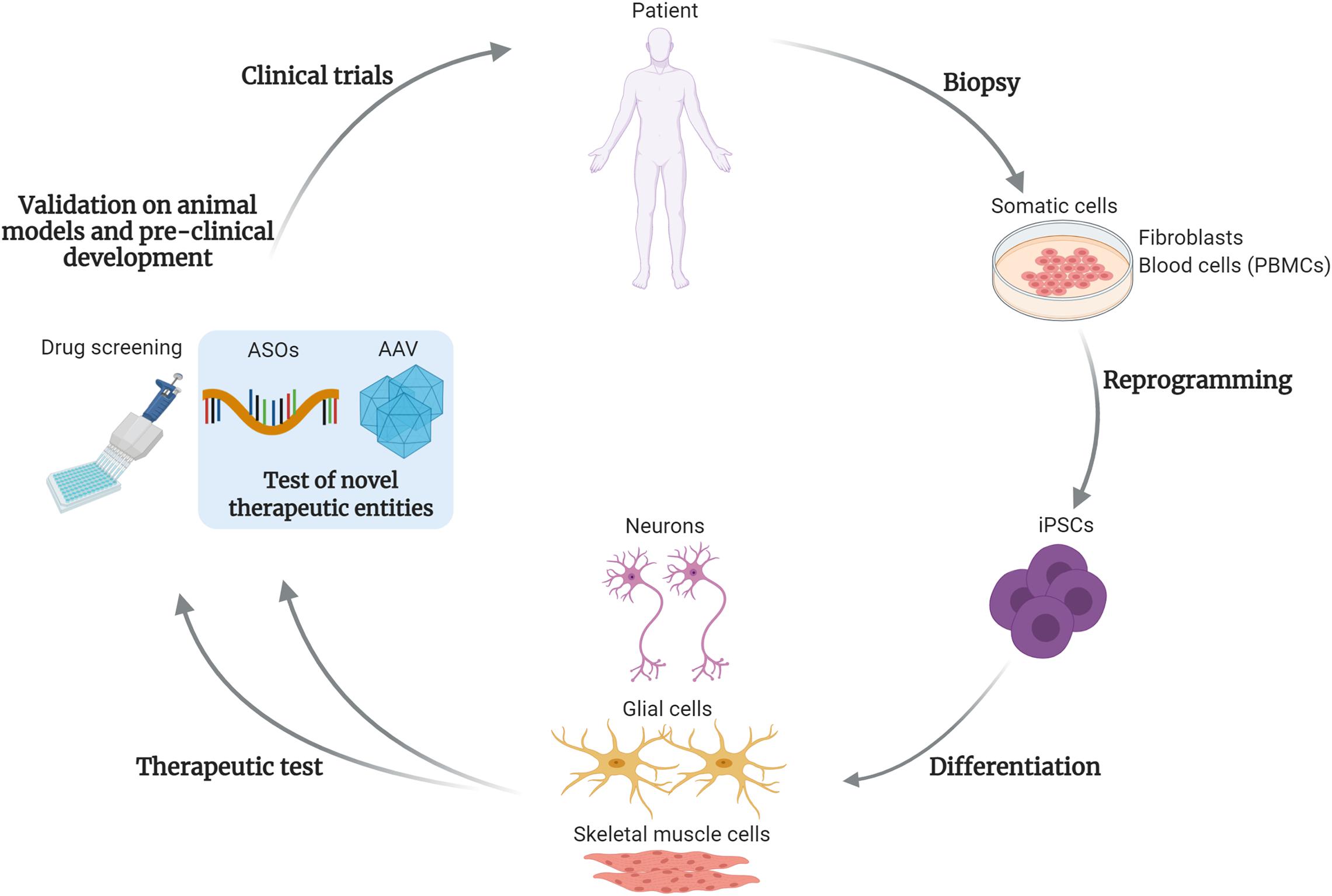
Induced Pluripotent Stem Cells (iPSCs)
iPSCs are reprogrammed adult cells capable of differentiating into various neural cell types. Their advantages include:
- Ability to generate patient-specific neural lineage cells
- Potential for controlled differentiation
- Reduced ethical concerns compared to embryonic sources
iPSC-derived neural progenitors can provide targeted neurotrophic support and enhance integration into damaged neural networks.
Below is a detailed, scientifically grounded explanation written in a professional tone.
Why Induced Pluripotent Stem Cells (iPSCs) May Have Greater Therapeutic Potential in ALS Compared to Mesenchymal Stem Cells (MSCs)
Both induced pluripotent stem cells (iPSCs) and mesenchymal stem cells (MSCs) have been investigated in ALS therapy. However, their biological roles and therapeutic capacities differ substantially. While MSCs are primarily immunomodulatory and supportive, iPSCs offer a broader regenerative and disease-modifying potential due to their pluripotency, neural differentiation capacity, and ability to generate disease-relevant cell types.
-
Pluripotency and Lineage Precision
The defining advantage of iPSCs lies in their pluripotent nature. iPSCs are reprogrammed adult somatic cells that regain the ability to differentiate into virtually any cell type in the body. In the context of ALS — a disease fundamentally characterized by degeneration of motor neurons and associated glial dysfunction — the ability to generate authentic neural lineage cells is critical.
MSCs derived from umbilical cord, bone marrow, or adipose tissue do not naturally differentiate into functional motor neurons or specialized glial cells in a controlled and stable manner. Their primary therapeutic mechanism is paracrine signaling — they release anti-inflammatory and trophic factors but rarely integrate structurally into neural circuits.
In contrast, iPSCs can be directed to become:
- Motor neuron progenitors
- Neuroblasts
- Oligodendrocyte precursor cells
- Astrocyte-supporting populations
This lineage specificity enables targeted replacement or reinforcement of cell types directly affected in ALS, addressing the root cellular pathology rather than only modulating the inflammatory environment.
-
Direct Motor Neuron Targeting
ALS pathology centers on progressive motor neuron degeneration in the spinal cord and motor cortex. MSCs are not inherently programmed to adopt a motor neuron phenotype. Even under neural induction conditions, MSC-derived “neuron-like” cells often lack full electrophysiological maturity and stable integration capacity.
iPSC-derived motor neurons, however, can be generated using defined differentiation protocols that mimic embryonic neural development. These cells express:
- HB9
- ISL1
- ChAT
- Other motor neuron–specific transcription factors
This allows for more precise cellular modeling and potentially more meaningful structural support to degenerating motor neuron pools.
Although full functional integration in ALS remains investigational, the biological plausibility of iPSC-derived motor neuron support is significantly stronger than that of MSC-derived substitutes.
-
Glial Cell Correction and Microenvironment Restoration
ALS is not purely a motor neuron disease. Astrocytes and oligodendrocytes play crucial roles in disease progression. Dysfunctional astrocytes can release toxic mediators, and oligodendrocyte impairment disrupts metabolic support to axons.
MSCs primarily influence glial cells indirectly via anti-inflammatory signaling. They reduce pro-inflammatory cytokines and shift microglial activation states, which is beneficial but not reconstructive.
iPSCs can generate:
- Oligodendrocyte precursor cells to support remyelination
- Astrocyte populations with corrected metabolic profiles
- Neural progenitor cells capable of integrating into the glial network
This allows for more comprehensive repair of the neural ecosystem rather than solely dampening inflammation.
-
Disease Modeling and Personalized Therapy
One of the most powerful advantages of iPSCs is their ability to be patient-specific. Cells can be reprogrammed from the patient’s own tissue, carrying the exact genetic mutations responsible for familial ALS (e.g., SOD1, C9orf72, TDP-43).
This provides two major benefits:
- Personalized therapeutic cell generation tailored to the patient’s biology.
- In vitro testing of differentiation quality and safety before transplantation.
MSCs, even when autologous, do not offer the same precision in modeling motor neuron pathology.
-
Axonal and Synaptic Support Capacity
ALS progression is closely linked to axonal degeneration and neuromuscular junction disruption. iPSC-derived neural progenitors demonstrate greater potential for:
- Axonal extension
- Synapse formation
- Production of neuron-specific adhesion molecules
MSCs mainly exert neuroprotective effects via secretion of BDNF, GDNF, and anti-inflammatory mediators, but they do not structurally contribute to axonal networks in a meaningful way.
-
Neurotrophic Profile Differences
While MSCs secrete neurotrophic factors, the neurotrophic profile of neural lineage cells derived from iPSCs is often more physiologically aligned with central nervous system repair. iPSC-derived neural cells produce growth factors in patterns more similar to native neural tissue.
Additionally, iPSC-derived exosomes may contain microRNAs and signaling molecules specifically involved in neuronal differentiation, axonal guidance, and synaptic plasticity — making their signaling more targeted toward neural repair pathways.
-
Strategic Therapeutic Positioning
Rather than viewing MSCs and iPSCs as competing technologies, many advanced protocols consider them complementary:
- MSCs: Strong immunomodulatory and anti-inflammatory support
- iPSCs: Structural neural lineage replacement and targeted regeneration
In ALS, where both neuroinflammation and direct motor neuron loss occur, iPSC-derived neural cells may offer a broader and more disease-specific regenerative strategy.
While both approaches remain investigational, iPSC-based strategies represent a more comprehensive attempt to address the underlying cellular pathology of ALS rather than solely modulating its inflammatory component.
Neural Lineage Cells: Targeted Precision
Rather than using undifferentiated cells alone, advanced protocols focus on specialized neural cells:
Neuroblasts
Immature neurons capable of differentiation. They support neuronal replacement strategies and enhance local signaling.
Axonal Support Cells
These cells enhance structural stability of motor neuron projections and help preserve neuromuscular connectivity.
Oligodendrocyte Precursors
Oligodendrocytes support myelin sheath integrity, which is crucial for efficient signal transmission along motor neurons.
The selection of these cells is strategic — ALS affects not only neurons but also supporting glial cells. Addressing the entire neural ecosystem increases therapeutic coherence.