Liver diseases are among the leading causes of death worldwide. Conditions such as fatty liver disease, hepatitis, fibrosis, and cirrhosis often progress silently and are diagnosed at advanced stages when treatment options are limited. In recent years, stem cell therapy has emerged as a promising regenerative treatment that may help restore liver function, reduce fibrosis, and improve quality of life for patients with chronic liver disease and cirrhosis.
This article explains the causes of liver damage, stages of disease progression, how stem cell therapy works, clinical outcomes, treatment protocol, costs, patient reviews, and answers to frequently asked questions.
The liver is a vital organ responsible for detoxification, metabolism, protein synthesis, and digestion support. Liver damage occurs when liver cells (hepatocytes) are continuously injured and replaced by fibrotic tissue. However, liver damage is not just the destruction of hepatocytes — it is a complex cellular process involving inflammation, immune response, and scar tissue formation.
Liver Structure and Main Cell Types
To understand liver damage, it is important to know the main liver cell types involved:
- Hepatocytes – main functional liver cells responsible for metabolism, detoxification, and protein synthesis.
- Kupffer cells – liver macrophages that regulate immune response and inflammation.
- Hepatic stellate cells – cells responsible for storing vitamin A and producing extracellular matrix; they play a key role in fibrosis.
- Endothelial cells – cells lining liver sinusoids and controlling blood flow and oxygen supply.
- Cholangiocytes – bile duct cells responsible for bile transport.
Liver disease develops when these cells are damaged and the normal regeneration process is disrupted.
The most common causes of liver damage include:
- Alcohol abuse – long-term alcohol consumption leads to alcoholic liver disease and cirrhosis.
- Viral hepatitis – hepatitis B, C, and D viruses cause chronic inflammation and fibrosis.
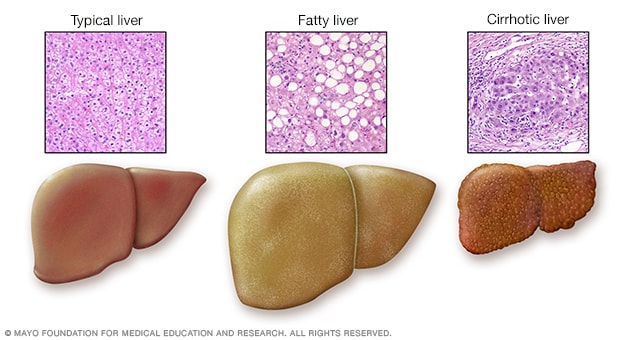
- Non-alcoholic fatty liver disease (NAFLD) – associated with obesity, diabetes, and metabolic syndrome.
- Drug toxicity – long-term use of certain medications damages hepatocytes.
- Autoimmune diseases – autoimmune hepatitis, primary biliary cholangitis.
- Genetic diseases – hemochromatosis, Wilson’s disease.
- Toxins and environmental exposure
- Poor diet and metabolic disorders
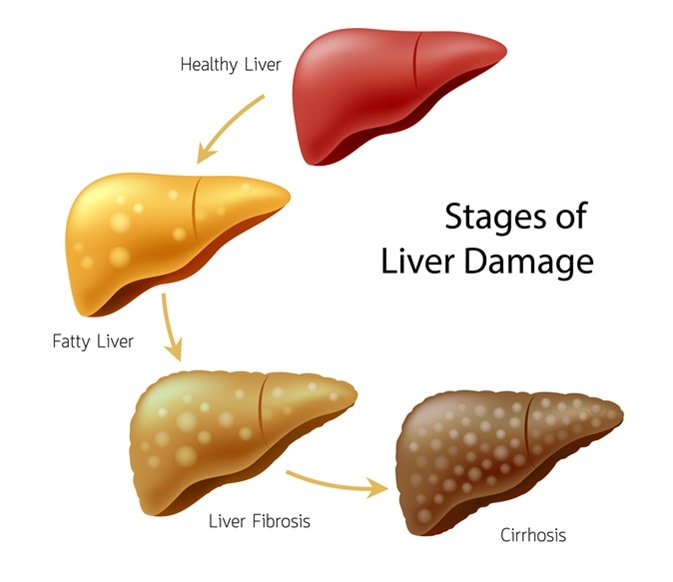
Chronic liver damage leads to fibrosis and eventually cirrhosis if untreated.
Step-by-Step Process of Liver Damage
1. Initial Hepatocyte Injury
Liver damage usually begins with injury to hepatocytes caused by:
- Alcohol/Viruses/Fat accumulation/ Toxins/ Drugs/ Autoimmune reactions
These factors cause:
- Oxidative stress/ Mitochondrial damage /Fat accumulation/ Cellular inflammati/ Cell death (apoptosis or necrosis)
When hepatocytes die, they release inflammatory signals.
2. Inflammation and Immune Response
After hepatocyte injury, Kupffer cells become activated and release:
- Cytokines/ Tumor necrosis factor (TNF)/ Interleukins/ Reactive oxygen species
This leads to chronic inflammation, which further damages hepatocytes and surrounding tissue.
If inflammation continues for a long time, the liver cannot regenerate properly.
3. Activation of Hepatic Stellate Cells – Beginning of Fibrosis
This is the most important step in liver fibrosis development.
When the liver is chronically injured:
- Hepatic stellate cells become activated
- They transform into myofibroblast-like cells
- These cells begin producing collagen and extracellular matrix
This collagen accumulates between liver cells and blood vessels.
As a result:
- Liver tissue becomes stiff/ Blood flow is impaired/ Oxygen supply decreases/ Hepatocytes die faster/ Regeneration becomes impaired
This process is called fibrosis.
4. Fibrosis Progression
Fibrosis progresses in stages:
- F1 – mild fibrosis
- F2 – moderate fibrosis
- F3 – severe fibrosis
- F4 – cirrhosis
During fibrosis:
- Normal liver tissue is replaced by scar tissue/ Liver structure changes/ Portal hypertension develops/ Liver function decreases
5. Cirrhosis – End Stage Liver Damage
Cirrhosis develops when fibrotic tissue completely disrupts liver architecture.
At this stage:
- Regenerative nodules form/ Blood cannot flow normally through the liver/ Detoxification decreases/ Protein synthesis decreases /Ascites may develop/ Portal hypertension develops/ Risk of liver cancer increases
Cirrhosis is considered irreversible in traditional medicine, but regenerative therapies such as stem cells aim to:
- Reduce fibrosis/Improve hepatocyte regeneration/Improve blood supply/Reduce inflammation/Improve liver function
Summary – Why Liver Damage Progresses
Liver damage progresses due to a cycle:
Hepatocyte injury → Inflammation → Stellate cell activation → Collagen production → Fibrosis → Cirrhosis → Liver failure
The key mechanism of liver disease progression is chronic inflammation and activation of hepatic stellate cells, which produce scar tissue instead of normal liver tissue.
GET FREE CONSULTATION

Liver disease progresses gradually through several stages, and at each stage specific biochemical, cellular, and functional changes occur. Understanding these changes helps explain why early treatment is critical and how regenerative therapies may help restore liver function.
Stage 1 – Inflammation (Hepatitis Stage)
What Happens at the Cellular Level
At the inflammation stage, hepatocytes are injured but most liver tissue is still functional. The damage is mainly caused by oxidative stress, fat accumulation, viral replication, toxins, or immune attack.
Biochemical processes:
- Increased oxidative stress
- Production of reactive oxygen species (ROS)
- Mitochondrial dysfunction in hepatocytes
- Activation of immune cells (Kupffer cells)
- Release of inflammatory cytokines:
- TNF-α
- IL-1
- IL-6
- Early hepatocyte apoptosis (programmed cell death)
Blood test changes:
- Increased ALT
- Increased AST
- Mild increase in GGT
- Sometimes increased bilirubin
- CRP may be elevated
Liver Function at This Stage
Liver function is mostly preserved because hepatocytes can still regenerate. Protein synthesis and detoxification are still normal.
Is this stage reversible?
Yes. If the cause of damage is removed (alcohol, virus, obesity, toxins), the liver can completely recover.
Stage 2 – Fibrosis (Scar Tissue Formation)
What Happens at the Cellular Level
At this stage, chronic inflammation activates hepatic stellate cells, which start producing collagen and extracellular matrix. Scar tissue begins to accumulate between hepatocytes and blood vessels.
Biochemical processes:
- Activation of stellate cells
- Increased collagen type I and III production
- Increased TGF-β (transforming growth factor beta) – main fibrosis signal
- Reduced matrix degradation (MMP/TIMP imbalance)
- Sinusoidal capillarization (loss of normal liver microcirculation)
- Reduced oxygen diffusion to hepatocytes
- Progressive hepatocyte death
Blood test changes:
- ALT and AST elevated
- GGT elevated
- Bilirubin may increase
- Albumin usually still normal
- Platelets may begin to decrease
- Fibrosis markers increase:
- Hyaluronic acid
- Procollagen III peptide
- FibroTest markers
Liver Function Changes
- Detoxification slightly reduced
- Fat metabolism impaired
- Bile flow may be impaired
- Glucose metabolism altered
- Mild insulin resistance may develop
At this stage, fibrosis can still be partially reversible if treatment reduces inflammation and fibrosis formation.
Stage 3 – Advanced Fibrosis
What Happens at the Cellular Level
Fibrotic tissue becomes widespread and starts disrupting liver architecture and blood flow.
Biochemical processes:
- Extensive collagen deposition
- Portal vein blood flow resistance increases
- Development of portal hypertension
- Reduced oxygen delivery to hepatocytes
- Hepatocyte regeneration becomes ineffective
- Formation of fibrotic septa
- Increased inflammation and oxidative stress
- Reduced nitric oxide production → impaired microcirculation
Blood test changes:
- ALT/AST may remain elevated or decrease (due to hepatocyte loss)
- Bilirubin increases
- Albumin begins to decrease
- Platelets decrease
- INR may increase
- Ammonia may increase
- Cholesterol synthesis decreases
Liver Function Changes
The liver begins to lose its major functions:
Detoxification decreases:
- Ammonia accumulates
- Toxins accumulate
- Risk of hepatic encephalopathy begins
Protein synthesis decreases:
- Albumin decreases
- Clotting factors decrease
- Edema and bleeding risk increase
Metabolism changes:
- Glucose regulation impaired
- Lipid metabolism impaired
- Hormone metabolism impaired
This stage is serious but still potentially manageable with regenerative and anti-fibrotic therapy.
Stage 4 – Cirrhosis
What Happens at the Cellular Level
Cirrhosis is the end stage of liver damage where normal liver tissue is replaced by fibrotic scar tissue and regenerative nodules.
Biochemical processes:
- Massive collagen accumulation
- Liver architecture completely disrupted
- Regenerative nodules form
- Severe portal hypertension
- Blood bypasses liver (portosystemic shunts)
- Severe hepatocyte loss
- Chronic inflammation continues
- Hypoxia in liver tissue
- Increased risk of hepatocellular carcinoma
- Reduced growth factor signaling
- Reduced hepatocyte proliferation
Blood test changes:
- High bilirubin
- Low albumin
- High INR
- Low platelets
- Elevated ammonia
- Low cholesterol
- Low urea production
- Electrolyte imbalance
- Elevated alkaline phosphatase
- MELD score increases
Liver Function at Cirrhosis Stage
Major liver functions are severely impaired:
| Liver Function | What Happens |
|---|---|
| Detoxification | Ammonia and toxins accumulate |
| Protein synthesis | Albumin and clotting factors decrease |
| Bile production | Fat digestion impaired |
| Hormone metabolism | Estrogen increases, testosterone decreases |
| Glucose metabolism | Hypoglycemia possible |
| Immune function | Infection risk increases |
| Blood filtration | Portal hypertension develops |
Clinical complications:
- Ascites
- Edema
- Varices
- Hepatic encephalopathy
- Bleeding
- Fatigue
- Muscle wasting
- Jaundice
Cirrhosis is traditionally considered irreversible, but modern regenerative medicine aims to:
- Reduce fibrosis
- Improve microcirculation
- Stimulate hepatocyte regeneration
- Improve liver synthetic function
- Reduce inflammation
Can Liver Disease Be Treated at Different Stages?
Early Stages (Inflammation)
Treatment focus:
- Remove cause of damage
- Antioxidants
- Anti-inflammatory therapy
- Metabolic correction
- Liver regeneration support
Fibrosis
Treatment focus:
- Anti-fibrotic therapy
- Improve microcirculation
- Reduce stellate cell activation
- Regenerative therapy (stem cells, exosomes)
- Hepatocyte support
Cirrhosis
Treatment focus:
- Improve remaining hepatocyte function
- Reduce portal hypertension
- Reduce inflammation
- Regenerative therapy
- Prevent complications
- Improve quality of life
End-Stage Liver Disease
Treatment options:
- Liver transplantation
- Bridging therapy with regenerative medicine
- Supportive therapy
Disease progression pathway:
Oxidative stress → Inflammation → Cytokines → Stellate cell activation → Collagen deposition → Fibrosis → Portal hypertension → Cirrhosis → Liver failure
Main biochemical changes during progression:
- Increased oxidative stress
- Increased inflammatory cytokines
- Increased collagen production
- Decreased albumin synthesis
- Increased bilirubin
- Increased ammonia
- Decreased detoxification
- Decreased clotting factors
- Impaired metabolism
- Portal hypertension
- Hypoxia in liver tissue


PREPARE AN INDIVIDUAL TREATMENT PLAN



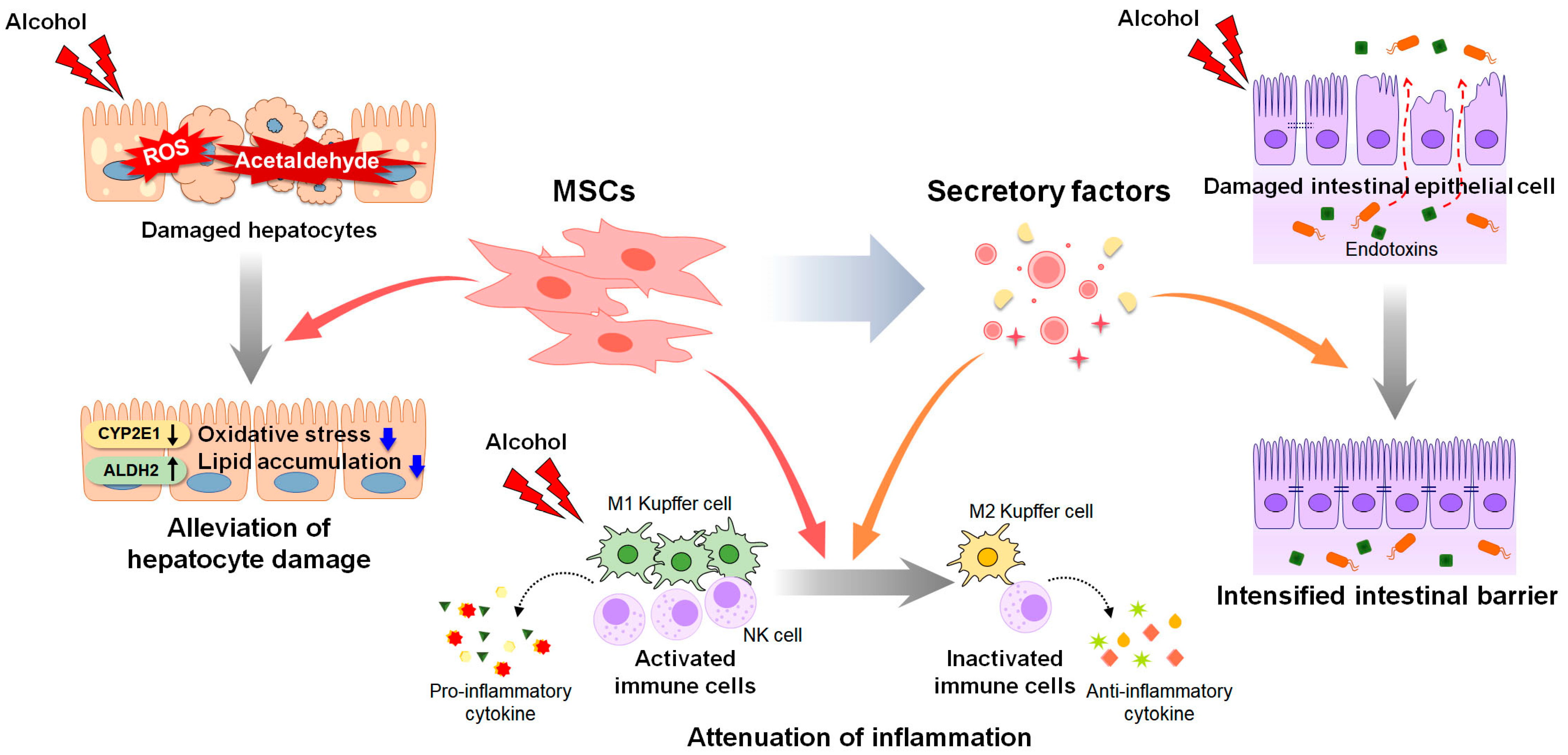
Clinical cases, observational programs, and regenerative medicine treatment protocols have demonstrated that stem cell therapy may lead to measurable improvements in liver function, fibrosis progression, and overall patient condition, particularly in patients with fibrosis and compensated cirrhosis. The therapeutic effect is not based on a single mechanism, but on a combination of anti-inflammatory, anti-fibrotic, angiogenic, and regenerative processes that gradually improve liver tissue structure and function.
One of the earliest changes observed after regenerative therapy is a reduction in liver inflammation. This is typically reflected by decreased levels of liver enzymes such as ALT (alanine aminotransferase) and AST (aspartate aminotransferase). These enzymes are markers of hepatocyte damage, and their reduction indicates decreased liver cell injury and improved hepatocyte stability.
Another important improvement is seen in bilirubin levels. Elevated bilirubin indicates impaired liver detoxification and bile metabolism. After regenerative therapy, many patients demonstrate gradual normalization or reduction of bilirubin levels, suggesting improved hepatocyte metabolic function and bile flow.
Albumin is one of the most important indicators of liver synthetic function. Since albumin is produced exclusively by hepatocytes, an increase in albumin levels after therapy suggests improved protein synthesis capacity of the liver and better overall liver function. This is particularly important in cirrhosis patients, where low albumin is associated with ascites, edema, and poor prognosis.
Stem cell therapy may also influence fibrosis progression. Over time, anti-fibrotic mechanisms, including inhibition of hepatic stellate cells and activation of matrix remodeling enzymes, may lead to reduced liver stiffness and improved liver elasticity measured by FibroScan or elastography. While complete reversal of cirrhosis is rare, fibrosis regression and stabilization are possible outcomes.
Clinical scoring systems such as the MELD score and Child-Pugh score are commonly used to assess liver disease severity and prognosis. Improvements in albumin, bilirubin, and INR values may lead to improved MELD and Child-Pugh scores, indicating better liver function and potentially improved survival prognosis.
Patients often report not only laboratory improvements but also clinical improvements, including reduced ascites, improved appetite, increased energy levels, better digestion, improved sleep, and overall better quality of life. Reduced hospitalization frequency is also an important clinical outcome, especially in patients with advanced liver disease.
It is important to understand that the degree of improvement depends on the stage of liver disease, underlying cause, patient age, metabolic condition, and lifestyle factors. Patients with fibrosis and early cirrhosis typically show better regenerative response compared to patients with end-stage liver failure.
Overall, stem cell therapy is considered relatively safe when performed under controlled clinical protocols, with most reported side effects being mild and transient, such as low-grade fever, fatigue, or infusion-related reactions.
Typical Laboratory and Clinical Changes After Stem Cell Therapy
Below is an example table of commonly observed changes in clinical and laboratory parameters after regenerative liver therapy.
Table: Clinical and Laboratory Improvements
| Parameter | Before Treatment | After Treatment (3–6 months) | Average Improvement |
|---|---|---|---|
| ALT | Elevated | Decreased | ↓ 30–50% |
| AST | Elevated | Decreased | ↓ 35–45% |
| Bilirubin | Elevated | Decreased | ↓ 30–40% |
| Albumin | Low | Increased | ↑ 25–30% |
| INR | Elevated | Improved | ↓ 20–30% |
| Platelets | Low | Increased | ↑ 30–35% |
| FibroScan (kPa) | High stiffness | Reduced stiffness | ↓ 30–40% |
| MELD Score | Moderate/High | Improved | ↓ 4–7 points |
| Child-Pugh Score | B/C | Improved | ↓ 2–3 points |
| Ascites | Present | Reduced | 50–60% reduction |
| Fatigue | Severe | Improved | 60–70% improvement |
| Quality of Life | Low | Improved | 60–70% improvement |
Average Clinical Outcomes Observed in Regenerative Liver Therapy Programs
Based on clinical observations and regenerative medicine programs, the following average outcomes are reported:
| Clinical Outcome | Percentage of Patients |
|---|---|
| Improvement in liver function tests | 70–80% |
| Stabilization of liver disease | 70–85% |
| Reduction in fibrosis progression | 50–60% |
| Improvement in MELD score | 50–65% |
| Reduction in ascites | 50–60% |
| Improved energy and quality of life | 60–80% |
| Reduced hospitalization rate | 40–50% |
| Overall clinical improvement | 65–85% |
Timeline of Expected Improvements
1 Month After Therapy
- Reduced inflammation
- Improved energy levels
- Mild improvement in ALT/AST
- Better appetite and digestion
3 Months After Therapy
- Improved albumin
- Reduced bilirubin
- Reduced ascites
- Improved metabolism
- Improved MELD/Child-Pugh in some patients
6 Months After Therapy
- Improved liver elasticity
- Fibrosis stabilization or reduction
- Improved protein synthesis
- Better overall liver function
- Improved quality of life
12 Months After Therapy
- Stabilization of disease progression
- Reduced complications
- Improved survival prognosis in some patients
- Possible need for repeat therapy depending on condition
Clinical results of stem cell therapy for liver disease typically include improvements in liver enzymes, bilirubin, albumin production, fibrosis markers, and liver stiffness. Many patients also experience improved MELD and Child-Pugh scores, reduced ascites, increased energy levels, and improved quality of life. While stem cell therapy is not a complete cure for cirrhosis, it may slow disease progression, improve liver function, reduce complications, and potentially delay the need for liver transplantation in selected patients.
Stem cell therapy for liver disease typically costs from 8,000 Euro, depending on the treatment protocol, number of cell components used, and the severity of the patient’s condition. The final treatment cost is usually determined after medical evaluation, laboratory tests, and review of the patient’s medical history and liver disease stage.
The cost of regenerative liver therapy is influenced by several important factors. One of the main factors is the stage of liver disease. Patients with early fibrosis usually require fewer cell infusions and a shorter treatment protocol, while patients with cirrhosis or advanced liver disease often require a more complex regenerative program with multiple cell types, higher cell doses, and longer monitoring. As a result, treatment for advanced liver disease is typically more expensive.
Another factor that affects the cost is the number and type of cellular products used in the therapy. A comprehensive regenerative protocol may include mesenchymal stem cells, iPSC-derived hepatocytes, endothelial cells, and exosomes. The inclusion of multiple regenerative components increases the complexity of cell preparation and laboratory processing, which influences the overall treatment cost.
The number of treatment sessions also plays a role in pricing. Some patients require a single treatment cycle, while others may require repeated infusions over several months depending on disease severity, fibrosis stage, and treatment response.
Hospital stay duration and level of medical supervision can also affect the total cost. Some treatment programs include inpatient monitoring for several days, intravenous infusions, imaging, and repeated laboratory tests to evaluate liver function and treatment safety.
Follow-up monitoring is another important component of regenerative therapy. After treatment, patients typically undergo follow-up blood tests, liver elastography (FibroScan), and medical consultations over several months to monitor liver regeneration, fibrosis progression, and overall health status.
What Is Usually Included in the Treatment Cost
The treatment price typically includes a comprehensive regenerative medicine program rather than only the stem cell injection procedure.
The treatment program usually includes:
- Initial medical consultation and case evaluation
- Review of medical history and previous tests
- Laboratory tests (blood tests, liver function tests, viral markers, coagulation tests)
- Stem cell and biological product preparation
- Mesenchymal stem cell therapy
- iPSC-derived hepatocyte therapy
- Endothelial cell therapy
- Exosome therapy
- Intravenous infusions and medical procedures
- Hospital stay (usually 3–5 days)
- Medical monitoring during therapy
- Discharge recommendations and medications
- Follow-up monitoring and consultations
Factors That Influence the Final Treatment Cost
The final cost of stem cell therapy for liver disease depends on several factors:
- Stage of liver disease (fibrosis vs cirrhosis)
- MELD and Child-Pugh score
- Number of stem cell doses required
- Use of hepatocytes derived from iPSC cells
- Use of endothelial cells and exosomes
- Duration of hospital stay
- Number of follow-up visits
- Individualized treatment protocol
- Need for repeated therapy cycles
- Patient’s overall health condition
Patients with advanced cirrhosis, ascites, portal hypertension, or severe fibrosis usually require more intensive regenerative therapy, which may increase the overall cost of treatment.
ARRANGE FREE CONSULTATION

Patient 1 – Ahmed R., Egypt
Diagnosis: Liver Cirrhosis secondary to Chronic Hepatitis C
Therapy: iPSC-derived hepatocytes + MSC + endothelial cells + exosomes (single infusion cycle)
Before Treatment:
- ALT: 145 U/L
- AST: 132 U/L
- Bilirubin: 2.8 mg/dL
- Albumin: 2.9 g/dL
- MELD score: 16
- Ascites: Moderate
6 Months After Therapy:
- ALT: 68 U/L
- AST: 55 U/L
- Bilirubin: 1.6 mg/dL
- Albumin: 3.6 g/dL
- MELD score: 11
- Ascites: Reduced
Patient Feedback: “I feel much more energetic and my appetite has improved. I can walk longer without fatigue, and my abdominal swelling is much less noticeable.”
Patient 2 – Maria S., Spain
Diagnosis: Non-Alcoholic Fatty Liver Disease (NAFLD) with Fibrosis F3
Therapy: Two cycles of MSC + iPSC-derived hepatocytes + exosomes
Before Treatment:
- Fibrosis: F3 (liver elastography)
- ALT: 120 U/L
- AST: 98 U/L
5 Months After Therapy:
- Fibrosis: F2
- ALT: 52 U/L
- AST: 44 U/L
Patient Feedback: “My metabolism feels better, and I’ve lost 6 kg. I no longer feel bloated after meals, and my energy during the day has significantly improved.”
Patient 3 – John K., USA
Diagnosis: Alcoholic Cirrhosis
Therapy: iPSC-hepatocytes + MSC + endothelial cells + exosomes, single infusion
Before Treatment:
- Severe fatigue
- Ascites: Moderate
- Albumin: 2.8 g/dL
4 Months After Therapy:
- Albumin: 3.5 g/dL
- Ascites: Mild
- Fatigue: Significantly improved
Patient Feedback: “I can finally go out for short walks without feeling exhausted. My swelling has reduced, and I feel much healthier overall.”
Patient 4 – Anna L., Germany
Diagnosis: Autoimmune Hepatitis
Therapy: MSC + iPSC-hepatocytes + exosomes, two infusion cycles
Before Treatment:
- Elevated ALT/AST
- Active inflammation markers
- Fibrosis F2
6 Months After Therapy:
- ALT/AST normalized
- Reduced inflammation markers
- Fibrosis stabilized
Patient Feedback: “My blood tests are much better, and I no longer have constant liver discomfort. I feel more energetic and my sleep has improved.”
Patient 5 – Rajesh P., India
Diagnosis: NAFLD with Fibrosis F2 and Insulin Resistance
Therapy: MSC + endothelial cells + exosomes
Before Treatment:
- ALT: 95 U/L
- AST: 80 U/L
- Ultrasound: Moderate fatty infiltration
- HbA1c: 7.2%
5 Months After Therapy:
- ALT: 50 U/L
- AST: 42 U/L
- Fatty infiltration: Reduced
- HbA1c: 6.5%
Patient Feedback: “My liver fat has decreased and my sugar levels are more stable. I feel lighter, and my digestion is much better.”
Patient 6 – Elena V., Russia
Diagnosis: Cirrhosis, Child-Pugh B
Therapy: Full regenerative protocol (iPSC-hepatocytes + MSC + endothelial cells + exosomes) over two cycles
Before Treatment:
- MELD: 14
- Frequent hospitalizations for ascites
- Low physical activity
6 Months After Therapy:
- MELD: 10
- Reduced hospitalization frequency
- Increased physical activity; able to walk 2 km without fatigue
Patient Feedback: “I feel stronger and can participate in daily activities again. My hospital visits have decreased, and I feel hopeful for the future.”
Patient 7 – Sophie M., France
Diagnosis: Drug-Induced Liver Injury (DILI)
Therapy: MSC + iPSC-hepatocytes + exosomes, single infusion
Before Treatment:
- ALT: 180 U/L
- AST: 160 U/L
- Fibrosis: F1–F2
- Fatigue: Severe
5 Months After Therapy:
- ALT: 52 U/L
- AST: 45 U/L
- Fibrosis: Reduced
- Energy levels: Significantly improved
Patient Feedback: “My liver tests are normal, and I feel much more active. I can focus on work again and no longer feel constantly tired.”
1. Can stem cells cure liver cirrhosis completely?
Stem cell therapy does not completely cure cirrhosis, especially in advanced stages where extensive fibrosis has occurred. However, it can significantly improve liver function, reduce inflammation, and slow or even partially reverse fibrosis. For many patients, therapy enhances quality of life and delays progression, sometimes reducing the need for a liver transplant. Early intervention offers the best chances of noticeable regenerative effects.
2. Is stem cell therapy safe?
When performed under controlled clinical protocols, stem cell therapy is generally considered safe. Mesenchymal stem cells and iPSC-derived hepatocytes have low immunogenicity and rarely cause severe complications. Mild, temporary side effects like low-grade fever, fatigue, or headache may occur but usually resolve quickly. Strict monitoring during infusion ensures patient safety.
3. How long do the results last?
The benefits of stem cell therapy typically last between 1.5 and 5 years, depending on the severity of liver disease, fibrosis stage, and overall patient health. Patients who maintain a healthy lifestyle and avoid hepatotoxic substances often experience longer-lasting improvements. Follow-up testing helps determine whether repeat therapy cycles are needed.
4. How many treatments are needed?
Most patients require 1–3 treatment cycles depending on the stage of liver disease and individual response. Early fibrosis may need only a single cycle, while advanced cirrhosis or complex cases may benefit from multiple sessions spaced several months apart. The treatment plan is customized based on lab results, imaging, and overall liver function.
5. Are the cells rejected by the body?
Mesenchymal stem cells (MSCs) and iPSC-derived hepatocytes are designed to be minimally immunogenic. This means the patient’s immune system usually does not recognize them as foreign, preventing rejection. In some protocols, additional supportive measures such as immunomodulatory exosomes are used to further reduce immune reactions.
6. When will I see improvement?
Many patients notice subtle improvements in energy, digestion, or appetite within 1–3 months after therapy. Laboratory improvements, such as lower liver enzymes and improved bilirubin or albumin, may become measurable within 2–6 months. Full regenerative effects, including fibrosis reduction and improved liver elasticity, are often observed at 6–12 months.
7. Can this therapy replace liver transplantation?
Stem cell therapy may delay the need for liver transplantation and improve liver function, but it does not always replace a transplant, especially in end-stage liver failure. Patients with moderate cirrhosis or fibrosis may stabilize and even improve significantly. In advanced cases, therapy can serve as a bridge to transplantation, improving patient condition and outcomes.
8. Are there side effects?
Side effects are usually mild and temporary, including low-grade fever, fatigue, mild headache, or infusion-site reactions. Serious complications are rare when therapy is administered under strict clinical protocols. Long-term safety has been supported by multiple clinical studies, but patients are closely monitored for any unexpected reactions.
9. Who is a good candidate for treatment?
Patients with liver fibrosis, compensated or decompensated cirrhosis, NAFLD/NASH, viral hepatitis, or drug-induced liver injury may benefit from stem cell therapy. Early-stage disease generally responds better, but even some advanced cases show improved liver function. Candidates must undergo a thorough medical evaluation to ensure they are suitable for regenerative therapy.
10. What lifestyle changes are required after treatment?
After stem cell therapy, patients should avoid alcohol and hepatotoxic medications to protect the regenerating liver. Maintaining a healthy weight, following a liver-friendly diet, and engaging in moderate physical activity supports long-term recovery. Regular follow-up tests are recommended to monitor liver function, and ongoing lifestyle management helps maximize therapeutic benefits.