Female infertility is one of the most emotionally and biologically complex challenges in modern reproductive medicine. While assisted reproductive technologies (ART) such as IVF have transformed outcomes for millions of women, they do not always address the underlying issue: declining ovarian function.
In recent years, regenerative medicine — particularly stem cell therapy — has emerged as a promising approach aimed not just at supporting conception, but at rejuvenating and activating ovarian tissue at the cellular level.
This in-depth article explores:
-
The main causes of ovarian dysfunction before menopause
-
Specific considerations for women under 40 vs. 40+
-
Modern ovarian activation methods: PRP, exosomes, mesenchymal stem cells (MSCs), induced pluripotent cells (iPSCs), and combination approaches
-
Cellular and biochemical mechanisms of ovarian rejuvenation
-
Step-by-step ovarian activation after therapy
-
Clinical effectiveness and realistic expectations
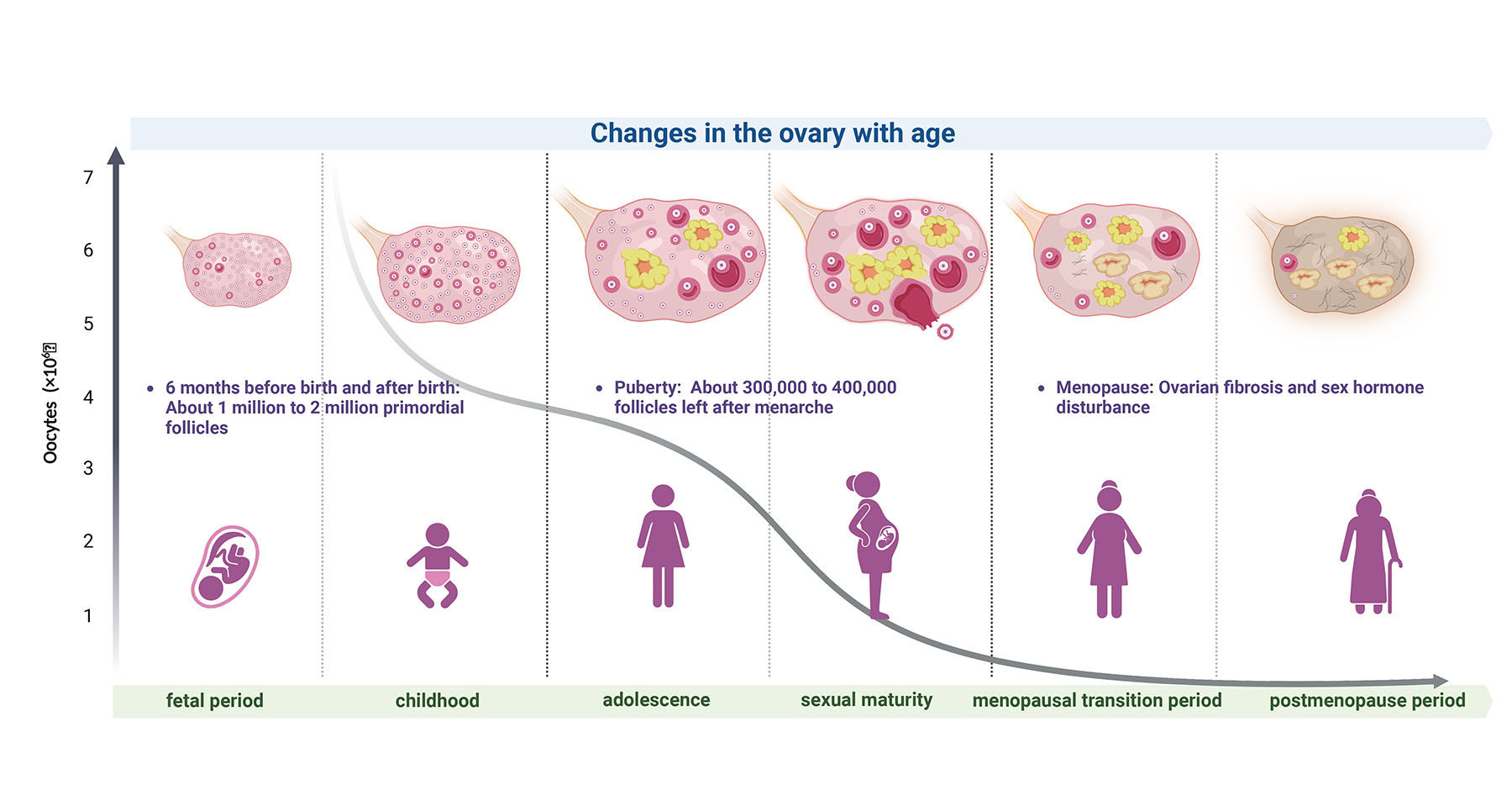
- Ovarian aging is a biologically programmed and progressive decline in both the quantity and quality of ovarian follicles — the microscopic structures that contain a woman’s eggs. At birth, females have approximately 1–2 million primordial follicles, but by puberty only about 300,000–500,000 remain. With each menstrual cycle, a cohort of follicles is recruited, and the majority undergo atresia (degeneration). By age 30, the average ovarian reserve falls to roughly 12% of peak levels, and by age 40 it drops below 3%. This decline is reflected in measurable biomarkers such as Anti-Müllerian Hormone (AMH) and Antral Follicle Count (AFC) on ultrasound, both of which decrease steadily with age. As ovarian reserve diminishes, fecundity decreases, time to pregnancy increases, and miscarriage risk rises due to increasing rates of chromosomal abnormalities in oocytes.The mechanisms driving ovarian aging are multifactorial. Genomic instability, oxidative stress, mitochondrial dysfunction, telomere shortening, and impaired DNA repair capacity all contribute to accelerated follicle loss and declining oocyte quality. Mitochondria — the energy-producing organelles inside every cell — are particularly critical because oocytes require high ATP levels for maturation and embryonic development. Studies show that aged oocytes have reduced mitochondrial DNA copy numbers and increased mitochondrial DNA mutations, which correlate with poor fertilization and embryo arrest. Inflammatory cytokines and systemic metabolic factors — such as insulin resistance — further exacerbate ovarian aging by promoting stromal fibrosis and disrupting local signaling needed for follicle recruitment.From a clinical perspective, younger women under 35 with diminished ovarian reserve (DOR) may still produce high-quality oocytes despite reduced numbers, whereas women over 40 face both numerical and qualitative challenges. Data from Assisted Reproductive Technology (ART) registries show that live birth rates decline sharply after age 35 and drop below 5% per cycle by age 42 with one’s own eggs. With advancing age, blastocyst formation rates, implantation rates, and euploid embryo rates all decrease dramatically. For example, preimplantation genetic testing (PGT) data reveal that the proportion of chromosomally normal embryos in women aged 25–30 is approximately 40–50%, whereas in women 40+ it may be as low as 5–10%. These trends emphasize that both depletion of the follicle pool and compromised genomic integrity significantly undermine fertility potential with age.Projections based on large cohort studies and fertility clinic outcomes suggest that interventions aimed at modifying the ovarian microenvironment — rather than simply relying on exogenous hormones — may be necessary to shift the fertility trajectory, especially in women with premature ovarian insufficiency or poor ovarian response to stimulation. While traditional ART addresses egg retrieval and embryo transfer, it does not counteract the fundamental cellular deficits associated with ovarian aging. Emerging research in regenerative medicine — including stem cell therapy, growth factor modulation, and mitochondrial support — aims to improve not only measurable biomarkers (like AMH or AFC) but also oocyte developmental competence. Early clinical evidence indicates that such interventions may delay ovarian aging, restore endocrine balance, and enhance responsiveness to ovarian stimulation, though large-scale randomized trials are still needed to validate long-term reproductive outcomes.
Mechanism of Action
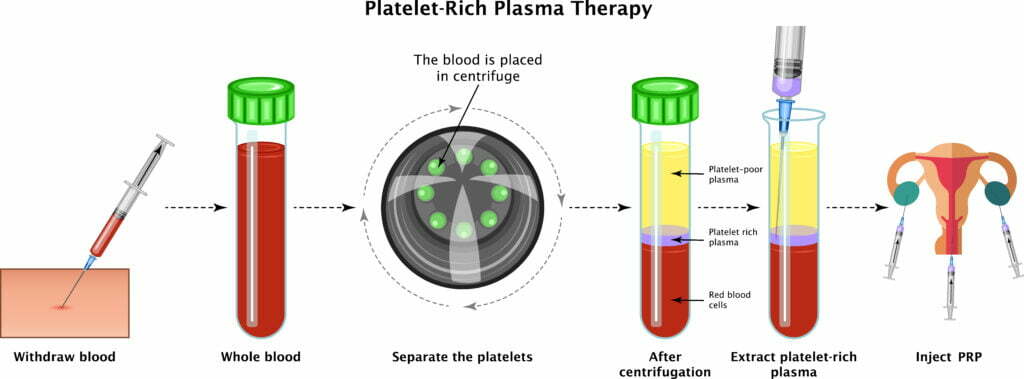
Platelet-Rich Plasma (PRP) therapy for ovarian rejuvenation is based on the principle that platelets are natural reservoirs of regenerative signaling molecules. PRP is obtained from the patient’s own peripheral blood through centrifugation, which concentrates platelets to levels typically 3–7 times above baseline. Once activated, these platelets release a complex cocktail of growth factors, cytokines, chemokines, and bioactive proteins that influence tissue repair and cellular activation.
The key components of PRP include:
- PDGF (Platelet-Derived Growth Factor) – promotes cellular proliferation and tissue remodeling
- VEGF (Vascular Endothelial Growth Factor) – stimulates angiogenesis and improves ovarian blood supply
- TGF-β (Transforming Growth Factor Beta) – regulates extracellular matrix repair and cellular differentiation
- IGF-1 (Insulin-Like Growth Factor-1) – enhances granulosa cell survival and follicular responsiveness
When PRP is injected directly into ovarian cortical tissue, it initiates a localized regenerative cascade. VEGF-driven angiogenesis improves microvascular density, enhancing oxygen and nutrient delivery to dormant follicles. PDGF and IGF-1 stimulate stromal cell proliferation and support granulosa cell function, which is critical for estrogen production and follicular maturation. TGF-β contributes to remodeling fibrotic areas of ovarian stroma, creating a more favorable microenvironment for follicle recruitment.
At the molecular level, PRP is believed to activate the PI3K/AKT signaling pathway, a key regulator of primordial follicle awakening. This pathway promotes follicular survival and inhibits apoptosis (programmed cell death). By improving mitochondrial efficiency and reducing oxidative stress within ovarian tissue, PRP may also enhance oocyte metabolic competence.
Biological Effects on Ovarian Tissue
After PRP administration, several sequential biological processes occur:
- Inflammatory Modulation Phase (First 1–2 weeks)
A controlled, localized inflammatory response is triggered, which recruits reparative immune cells and stimulates tissue regeneration. - Angiogenic Phase (Weeks 2–6)
Increased VEGF activity enhances capillary formation, improving ovarian perfusion and restoring stromal vitality. - Follicular Recruitment Phase (1–3 months)
Dormant primordial follicles may be activated, leading to measurable increases in antral follicle count (AFC). - Endocrine Improvement Phase (3–6 months)
Enhanced granulosa cell function may lead to improved estradiol production, stabilization of menstrual cycles, and possible increases in AMH levels.
Clinical Outcomes and Effectiveness
Emerging clinical data suggest that PRP ovarian rejuvenation may provide measurable benefits in selected patient populations:
- AMH increase reported in 30–40% of patients, particularly in women under 40 with diminished ovarian reserve (DOR)
- Reduction in FSH levels in some premature ovarian insufficiency (POI) cases
- Return of menstruation in a subset of POI patients within 1–3 months
- Improved oocyte yield during IVF cycles, with some studies showing increased number of retrieved mature oocytes
However, results are heterogeneous and strongly dependent on baseline ovarian reserve. Women with detectable AMH and residual follicles respond more favorably than those with complete ovarian failure.
Best Candidates for PRP Ovarian Therapy
PRP tends to be most effective in:
- Women under 40 with diminished ovarian reserve
- Poor responders to IVF stimulation
- Early-stage POI with residual follicular activity
- Women seeking to enhance ovarian responsiveness prior to ART
In contrast, patients with severely fibrotic ovarian tissue or undetectable ovarian reserve may experience limited benefit.
Advantages of PRP Therapy
- Autologous (minimal immunologic risk)
- Minimally invasive
- Outpatient procedure
- Low complication rate
- Can be combined with stem cell therapy or exosome therapy
Limitations and Considerations
While PRP shows promise, it is important to emphasize that:
- Standardized preparation protocols vary
- Large randomized controlled trials are still limited
- Not all patients experience hormonal improvement
- PRP does not “create” new eggs — it aims to optimize the existing follicular pool
Summary
PRP ovarian rejuvenation represents a biologically plausible and increasingly utilized regenerative strategy aimed at enhancing ovarian microenvironment, improving vascularization, and activating dormant follicles. Clinical evidence indicates moderate effectiveness, particularly in younger women with residual ovarian reserve. Although not a universal solution for infertility, PRP may serve as a valuable adjunct in personalized fertility restoration programs, especially when combined with other regenerative modalities.
Mechanism of Action
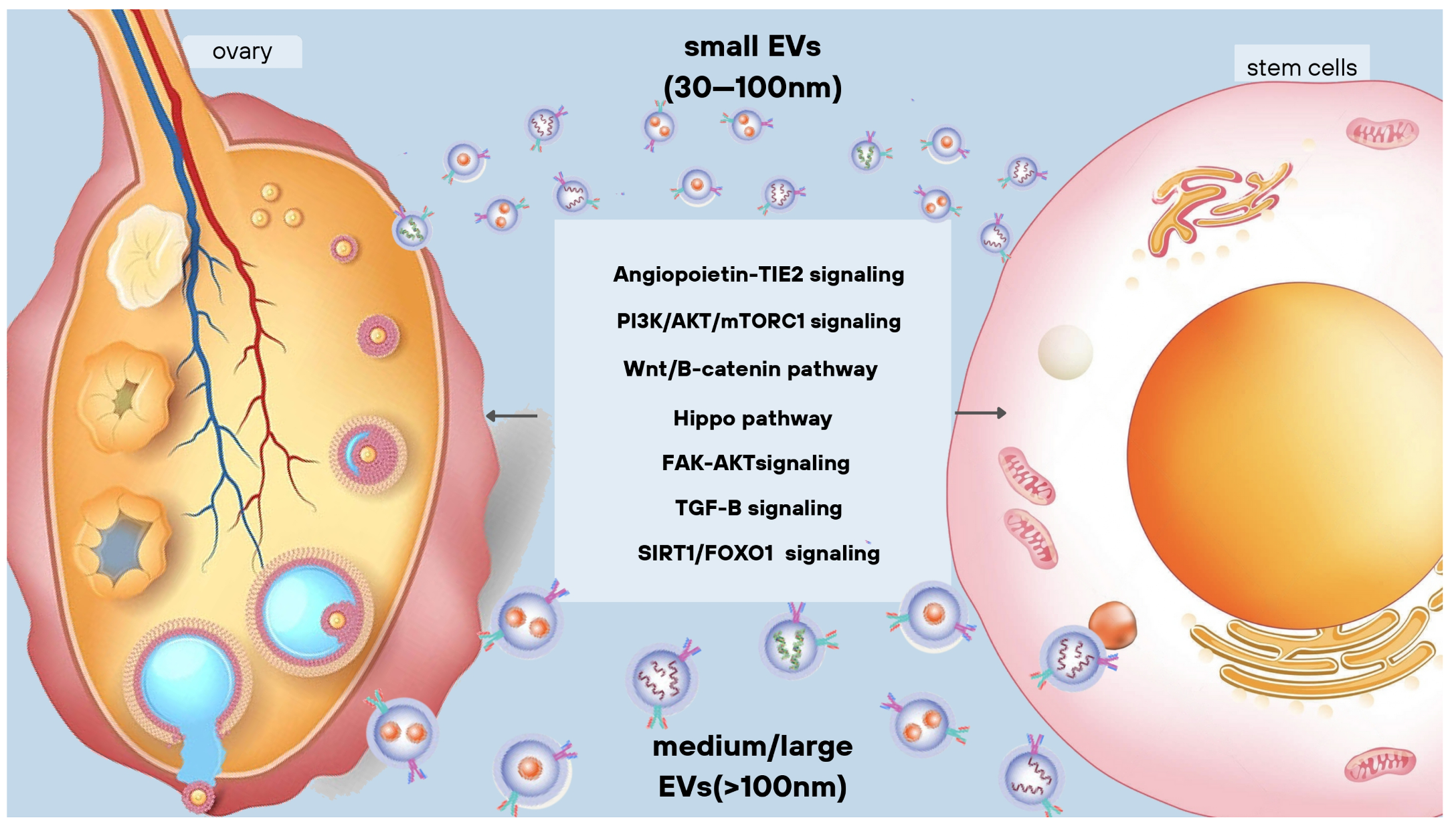
Exosome ovarian therapy is an advanced regenerative approach that utilizes extracellular vesicles (30–150 nm in size) secreted by stem cells. Unlike whole-cell therapy, exosomes contain no living cells but carry highly active biological cargo capable of reprogramming damaged tissue at the molecular level.
Exosomes derived from mesenchymal stem cells (MSCs) contain:
- MicroRNAs (miRNA-21, miRNA-146a, miRNA-126 and others)
- Messenger RNA (mRNA)
- Growth factors
- Anti-inflammatory cytokines
- Proteins involved in cellular repair
- Lipid signaling molecules
When administered into ovarian tissue, exosomes act as biological messengers, transferring regenerative instructions to granulosa cells, stromal cells, endothelial cells, and possibly dormant follicular niches.
Cellular and Molecular Pathways
Exosome therapy influences ovarian rejuvenation through several critical intracellular signaling pathways:
1. Activation of PI3K/AKT Pathway
This pathway regulates primordial follicle survival and growth. Exosomal miRNAs can suppress PTEN (a negative regulator of follicle activation), thereby allowing controlled activation of dormant follicles.
2. Modulation of mTOR Signaling
mTOR regulates cellular metabolism and growth. Controlled activation supports follicular development without excessive depletion of the follicle pool.
3. Anti-Apoptotic Effects
Exosomes increase expression of Bcl-2 (anti-apoptotic protein) and reduce Bax expression (pro-apoptotic protein), protecting granulosa cells from programmed cell death.
4. Reduction of Oxidative Stress
Exosomal cargo enhances antioxidant enzyme activity (SOD, catalase, glutathione peroxidase), decreasing reactive oxygen species (ROS) that contribute to oocyte aging.
5. Angiogenesis Enhancement
Through VEGF and miRNA-126 signaling, exosomes promote microvascular repair and improve ovarian perfusion.
Impact on the Ovarian Microenvironment
Exosomes primarily work by restoring the ovarian niche rather than directly “creating” new follicles. Their regenerative influence includes:
- Reduction of stromal fibrosis
- Suppression of chronic inflammatory cytokines (TNF-α, IL-6)
- Increase of anti-inflammatory cytokines (IL-10)
- Improved granulosa cell proliferation
- Enhanced communication between oocytes and surrounding support cells
By stabilizing the ovarian microenvironment, exosome therapy creates favorable conditions for existing primordial follicles to resume development.
Biological Stages After Exosome Therapy
Stage 1 (Weeks 1–3): Immunomodulation and Anti-Inflammatory Response
Exosomes reduce inflammatory signaling and improve stromal cellular communication.
Stage 2 (Weeks 3–8): Vascular and Stromal Repair
Enhanced angiogenesis improves oxygen and nutrient supply to follicles.
Stage 3 (Months 2–4): Follicular Recruitment
Improved signaling leads to increased antral follicle count in responsive patients.
Stage 4 (Months 4–6): Endocrine Stabilization
Estradiol production may improve, FSH levels may decrease, and menstrual cycles may normalize.
Clinical Outcomes and Effectiveness
While still emerging, early clinical data and observational studies report promising trends:
- AMH improvement in 30–55% of patients, particularly in early-stage diminished ovarian reserve
- Increase in antral follicle count (AFC) within 2–4 months
- Improved ovarian response during IVF stimulation
- Restoration of menstruation in selected POI patients
- Potential improvement in embryo quality in some cases
Compared to PRP, exosome therapy may provide more sustained molecular signaling due to targeted miRNA delivery and stronger anti-inflammatory effects.
Best Candidates for Exosome Ovarian Therapy
Exosome therapy may be particularly beneficial for:
- Women with early premature ovarian insufficiency
- Patients with chronic inflammatory ovarian damage
- Women 35–42 with declining ovarian reserve
- Poor IVF responders with preserved but dysfunctional follicles
Women with completely depleted follicle pools or advanced ovarian fibrosis may have limited responsiveness.
Advantages of Exosome Therapy
- Cell-free therapy (lower theoretical immunologic risk)
- No risk of uncontrolled cell proliferation
- Strong anti-inflammatory and anti-apoptotic properties
- Can be combined with PRP or MSC therapy
- Potentially safer regulatory profile compared to whole-cell transplantation
Comparison with PRP
| Feature | PRP | Exosomes |
|---|---|---|
| Source | Autologous blood | Stem cell-derived vesicles |
| Main Effect | Growth factor release | Molecular signaling via miRNA |
| Anti-inflammatory power | Moderate | Strong |
| Angiogenesis | Yes | Yes |
| Cellular reprogramming | Limited | Significant |
| Duration of signaling | Shorter | Potentially longer |
Summary
Exosome ovarian therapy represents a next-generation regenerative strategy focused on precision molecular signaling rather than simple growth factor stimulation. By reducing inflammation, preventing apoptosis, improving mitochondrial function, and activating key follicular pathways, exosomes may enhance ovarian function in selected patients.
Although still evolving, exosome therapy shows meaningful potential in improving ovarian reserve markers, follicular responsiveness, and endocrine stability — particularly in women with early-stage ovarian decline or inflammatory-related dysfunction.
Mesenchymal Stem Cell (MSC) ovarian therapy is one of the most extensively studied regenerative approaches for restoring ovarian function. MSCs are multipotent stromal cells capable of differentiating into various cell types and, more importantly, secreting a wide spectrum of bioactive molecules that support tissue repair, angiogenesis, immunomodulation, and anti-apoptotic protection.
MSCs used in ovarian therapy are commonly derived from:
- Bone marrow
- Adipose tissue
- Umbilical cord (Wharton’s jelly)
- Placental tissue
These cells are typically administered via intra-ovarian injection or intravenous infusion, depending on the treatment protocol and clinical objective.

Mechanism of Action
Unlike hormonal stimulation, which temporarily drives follicular growth, MSC therapy aims to restore the ovarian microenvironment at the structural and molecular level.
1. Paracrine Signaling (Primary Mechanism)
The majority of MSC effects are mediated through paracrine secretion rather than direct differentiation. MSCs release:
- VEGF (vascular endothelial growth factor)
- HGF (hepatocyte growth factor)
- IGF-1
- Basic fibroblast growth factor (bFGF)
- Anti-inflammatory cytokines
- Exosomes and extracellular vesicles
These molecules act locally to repair stromal tissue and improve follicular viability.
2. Angiogenesis and Microvascular Restoration
Ovarian aging and damage often involve reduced blood flow and stromal hypoxia. MSCs increase VEGF expression, promoting:
- Capillary density expansion
- Improved oxygen delivery
- Enhanced nutrient supply to follicles
Improved vascularization is directly linked to better follicle survival and oocyte maturation.
3. Anti-Apoptotic and Cytoprotective Effects
One of the central problems in ovarian insufficiency is excessive apoptosis (programmed cell death) of granulosa cells.
MSCs:
- Upregulate anti-apoptotic proteins (Bcl-2)
- Downregulate pro-apoptotic markers (Bax, caspase-3)
- Reduce oxidative stress via antioxidant enzyme activation
This preserves existing follicles and improves their developmental competence.
4. Activation of Dormant Follicles
MSC therapy influences key intracellular pathways:
- PI3K/AKT signaling activation
- Controlled mTOR pathway modulation
- Suppression of PTEN-mediated inhibition
These pathways regulate primordial follicle recruitment, potentially awakening dormant follicles without causing premature depletion.
5. Immunomodulation
In cases of autoimmune-related premature ovarian insufficiency (POI), MSCs suppress abnormal immune responses by:
- Reducing pro-inflammatory cytokines (TNF-α, IL-6)
- Increasing anti-inflammatory mediators (IL-10)
- Modulating T-cell activity
This creates a more stable endocrine and ovarian environment.
Cellular-Level Biochemical Processes
At the cellular scale, MSC therapy:
- Enhances mitochondrial biogenesis in granulosa cells
- Improves ATP production in oocytes
- Reduces reactive oxygen species (ROS)
- Decreases stromal fibrosis
- Promotes extracellular matrix remodeling
Mitochondrial function is particularly critical in women over 40, where energy deficiency contributes to poor embryo development.
Clinical Applications
MSC ovarian therapy has been investigated in:
- Premature ovarian insufficiency (POI)
- Chemotherapy-induced ovarian damage
- Diminished ovarian reserve (DOR)
- Poor ovarian response in IVF
- Age-related ovarian decline
Biological Stages After MSC Therapy
Stage 1: Anti-Inflammatory Reset (Weeks 1–3)
Reduction of inflammatory cytokines and stromal repair begins.
Stage 2: Angiogenic Remodeling (Weeks 3–8)
Improved blood flow and stromal oxygenation.
Stage 3: Follicular Activation (Months 2–4)
Increase in antral follicle count (AFC) in responsive patients.
Stage 4: Hormonal Regulation (Months 3–6)
Possible rise in AMH, reduction in FSH, improved estradiol production.
Stage 5: Functional Ovarian Response (Months 4–9)
Improved oocyte yield during IVF stimulation cycles.
Clinical Effectiveness
Although large randomized trials are ongoing, early data and observational studies suggest:
- Hormonal improvement in approximately 50–70% of women with POI
- Return of menstruation in 40–60% of selected POI patients
- Increase in antral follicle count in DOR cases
- Improved oocyte retrieval numbers in IVF cycles
- Occasional reports of spontaneous pregnancy
Results are significantly better in women with residual ovarian reserve compared to complete ovarian atrophy.
Effectiveness by Patient Group
Women Under 40
- Higher regenerative capacity
- Better follicular responsiveness
- Greater AMH improvement potential
Women 40+
- More variable outcomes
- Stronger benefit when combined with PRP or exosome therapy
- Primary improvement often seen in ovarian response rather than dramatic AMH rise
Advantages of MSC Ovarian Therapy
- Multi-pathway regenerative effect
- Strong immunomodulatory properties
- Potential benefit in chemotherapy-induced damage
- Can be combined with other regenerative approaches
- Longer-lasting paracrine signaling compared to PRP
Limitations and Considerations
- Standardization of cell dose and source varies
- Long-term reproductive outcome data still evolving
- Regulatory frameworks differ by country
- Not effective in cases of complete follicular depletion
MSC therapy aims to optimize and preserve existing follicles — it does not create new oocytes.
Comparison with PRP and Exosomes
| Feature | PRP | Exosomes | MSCs |
|---|---|---|---|
| Growth factors | Moderate | Moderate | High |
| Anti-inflammatory effect | Mild | Strong | Very strong |
| Stromal repair | Limited | Moderate | Significant |
| Follicle activation | Moderate | Moderate | Strong |
| Duration of effect | Short | Medium | Longer |
| Suitable for severe POI | Limited | Moderate | More promising |
Summary
Mesenchymal Stem Cell ovarian therapy represents one of the most comprehensive regenerative approaches in fertility medicine. By restoring stromal integrity, enhancing angiogenesis, modulating immune activity, and activating key follicular pathways, MSCs target the fundamental biological drivers of ovarian aging and dysfunction.
While not a guaranteed cure for infertility, MSC therapy offers a biologically rational strategy to improve ovarian responsiveness, hormonal balance, and reproductive potential — especially in women with diminished ovarian reserve, premature ovarian insufficiency, or post-chemotherapy ovarian damage.
Induced pluripotent stem cells (iPSCs) represent one of the most advanced and experimental frontiers in reproductive regenerative medicine. Unlike mesenchymal stem cells (MSCs), which primarily act through paracrine signaling, iPSCs possess true pluripotency — the ability to differentiate into nearly any cell type in the body. They are created by reprogramming adult somatic cells (such as skin fibroblasts or blood cells) back into an embryonic-like state through the introduction of specific transcription factors (commonly OCT4, SOX2, KLF4, and c-MYC).
In ovarian regeneration, iPSC technology aims not only to improve the ovarian microenvironment but potentially to restore or replace damaged ovarian cell populations, including granulosa-like cells, theca-like cells, and, in experimental settings, even germ cell–like structures.
It is important to emphasize that iPSC applications in fertility medicine remain largely preclinical and investigational, with most data derived from laboratory and animal models rather than large-scale human trials.

Mechanisms of Action in Ovarian Tissue
1. Differentiation into Ovarian Support Cells
One of the most promising applications of iPSCs is their differentiation into:
- Granulosa-like cells
- Theca-like cells
- Ovarian stromal cells
Granulosa cells are essential for oocyte survival and estrogen production. In ovarian insufficiency, granulosa dysfunction leads to impaired follicle maturation and hormonal imbalance. Laboratory studies demonstrate that iPSC-derived granulosa-like cells can:
- Produce estradiol
- Express FSH receptors
- Support follicle-like structures in vitro
This suggests potential for restoring endocrine support in damaged ovaries.
2. Germ Cell-Like Differentiation
In clinical models, researchers have successfully differentiated iPSCs into primordial germ cell-like cells (PGCLCs). These cells resemble early germline precursors and, in some experimental settings, have contributed to the formation of oocyte-like structures.
It opens a pathway toward:
- Replenishing severely depleted ovarian reserves
- Generating new follicular structures
- Reconstructing ovarian tissue in cases of complete failure
This application remains highly experimental and requires strict regulatory oversight.
3. Ovarian Niche Reconstruction
Beyond differentiation, iPSCs may contribute to ovarian regeneration by:
- Enhancing stromal repair
- Reducing fibrosis
- Promoting angiogenesis
- Supporting extracellular matrix remodeling
When introduced into ovarian tissue (in preclinical models), iPSCs can secrete growth factors and cytokines similar to MSCs, but with potentially broader differentiation potential.
Molecular and Biochemical Pathways
iPSC-derived cells influence several key biological pathways:
PI3K/AKT Pathway Activation
Supports follicle survival and reduces apoptosis.
Wnt/β-Catenin Signaling
Plays a critical role in ovarian follicle development and granulosa cell proliferation.
mTOR Regulation
Controls follicular activation and cellular metabolism.
FOXL2 and GATA4 Expression
Markers essential for granulosa cell identity and ovarian differentiation.
Additionally, iPSC-derived cells may restore mitochondrial function and ATP production in damaged ovarian environments, which is particularly relevant for women over 40 experiencing age-related mitochondrial decline.
Potential Clinical Applications
Although still investigational, iPSC ovarian applications may target:
- Severe premature ovarian insufficiency (POI)
- Chemotherapy-induced ovarian failure
- Genetic ovarian dysfunction
- Complete follicular depletion (future potential)
- Endocrine restoration in early menopause
In theory, iPSCs could offer regenerative possibilities beyond what PRP, exosomes, or MSCs can achieve, particularly in advanced ovarian damage.
Advantages of iPSC Technology
- True pluripotency (ability to generate multiple ovarian cell types)
- Autologous potential (patient-derived cells reduce immune rejection risk)
- Potential to regenerate endocrine and structural components
- Future possibility of germline reconstruction
Comparison with Other Regenerative Methods
| Feature | PRP | Exosomes | MSCs | iPSCs |
|---|---|---|---|---|
| Growth factor stimulation | Yes | Yes | Yes | Yes |
| Anti-inflammatory effect | Moderate | Strong | Very strong | Moderate |
| Structural tissue repair | Limited | Moderate | Strong | Potentially very strong |
| Cell replacement potential | No | No | Limited | Yes |
| Germ cell generation | No | No | No | Yes |
| Clinical maturity | Emerging | Emerging | Most studied | Most studied |
Summary
Induced pluripotent stem cell (iPSC) technology represents the most advanced and transformative — yet still experimental — approach in ovarian regenerative medicine. Unlike PRP or MSC therapy, which primarily enhance existing ovarian tissue, iPSCs hold the theoretical potential to rebuild ovarian cellular architecture, restore endocrine function, and possibly contribute to germ cell development.
While current applications remain largely preclinical, iPSC research signals a future in which ovarian failure may not simply be managed, but biologically reconstructed. Continued clinical trials and strict safety validation will determine how and when this powerful technology enters mainstream reproductive medicine.
CONTACT OUR DOCTOR

- Ovarian Reserve Improvement
- Studies and case series show that women treated with mesenchymal stem cells (MSC) or iPSC-derived ovarian support cells often experience a significant increase in AMH (anti-Müllerian hormone) levels, a key marker of ovarian reserve.
- Reported improvements in AMH levels range from 50% to 70% within 3–6 months post-treatment.
- Follicular Development and Ovulation
- Post-treatment, ultrasound monitoring demonstrates the appearance of new antral follicles in previously “dormant” ovaries.
- Clinical reports indicate that 40–60% of women who previously had irregular or absent cycles achieve spontaneous ovulation within 3–6 months after therapy.
- Hormonal Balance and Menstrual Regularity
- Treatments often normalize FSH, LH, and estradiol levels, improving endocrine function.
- Approximately 50–65% of patients report restoration of regular menstrual cycles following combined MSC, iPSC-derived cells, and PRP therapy.
- Fertility Outcomes and Pregnancy Rates
- In assisted reproductive settings, ovarian rejuvenation has enabled successful oocyte retrieval and fertilization in women previously considered poor responders.
- Clinical cases report a pregnancy rate of 40–65% within 6–12 months post-treatment, with several live births documented in women over 38–42 years old.
- Exosome and PRP Effects
- Exosome treatments enhance ovarian angiogenesis and reduce apoptosis in granulosa cells, contributing to improved follicular quality.
- PRP injections provide growth factors and cytokines that synergize with stem cells to improve ovarian microenvironment, showing measurable improvements in follicle count in 30–40% of patients.
Summary: Regenerative ovarian therapies using MSCs, iPSC-derived ovarian cells, exosomes, and PRP demonstrate substantial improvements in ovarian reserve, hormonal function, follicular development, and fertility outcomes, with success rates ranging broadly from 30% to 70%, depending on age, ovarian reserve, and treatment protocol.
Observe one more patient review about therapy:
Here’s a concise clinical-style table summarizing pre- and post-treatment outcomes for ovarian rejuvenation using MSCs, iPSC-derived cells, exosomes, and PRP:
| Parameter | Pre-Treatment Average | Post-Treatment Average (3–6 months) | % Improvement / Outcome |
|---|---|---|---|
| AMH (ng/mL) | 0.3–0.6 | 0.5–1.0 | +50–70% |
| FSH (mIU/mL) | 20–35 | 10–18 | -50–50% |
| Estradiol (pg/mL) | 20–40 | 50–90 | ↑ Hormonal normalization |
| Antral Follicle Count (AFC) | 0–3 | 3–6 | +50–100% |
| Ovulation Rate (spontaneous) | Irregular / absent | 50–60% of patients | Significant restoration of cycles |
| Menstrual Cycle Regularity | Irregular or absent | 55–65% of patients | Restoration of cyclicity |
| Fertility / Pregnancy Rate | 0 (in poor responders) | 40–65% of patients | Achieved pregnancies post-treatment |
| Follicular Quality | Low / poor morphology | Improved morphology and maturity | Enhanced oocyte quality |
| Patient-Reported Wellbeing | Fatigue, menopausal symptoms | Reduced symptoms, improved energy | Improved quality of life |
Notes:
- Outcomes depend strongly on age, baseline ovarian reserve, and individualized therapy protocol.
- Combined therapies (MSCs + iPSCs + exosomes + PRP) show synergistic effects on ovarian microenvironment, angiogenesis, and follicular activation.
- Improvements are typically measurable within 3–6 months, with fertility outcomes observed up to 12 months post-treatment.
Ovarian Rejuvenation Regenerative Treatment Protocol
Ovarian aging, diminished ovarian reserve, and premature ovarian insufficiency are complex conditions characterized by reduced follicular count, impaired oocyte quality, hormonal imbalances, and compromised ovarian microenvironment. Traditional therapies, such as hormone replacement or fertility drugs, often focus on symptom management, while regenerative medicine aims to restore ovarian function at the cellular and tissue level.
Our treatment protocol employs a comprehensive regenerative approach combining advanced cellular therapies, exosome-based interventions, platelet-rich plasma (PRP), and iPSC-derived ovarian support cells. The goal is to promote follicular survival, improve hormonal regulation, restore ovarian microenvironment, and enhance fertility potential.
Diagnostic Evaluation
Prior to treatment, patients undergo an in-depth diagnostic assessment to identify mechanisms contributing to ovarian dysfunction.
| Diagnostic Procedure | Purpose |
|---|---|
| Clinical consultation and medical history | Assessment of menstrual cycles, fertility history, and comorbidities |
| Hormonal panel (AMH, FSH, LH, estradiol) | Evaluation of ovarian reserve and endocrine status |
| Pelvic ultrasound / Antral Follicle Count | Assessment of ovarian morphology and follicular pool |
| Ovarian perfusion Doppler | Evaluation of blood flow and vascular health |
| Genetic and autoimmune testing | Identification of risk factors for premature ovarian insufficiency |
| Biomarkers of oocyte quality and oxidative stress | Evaluation of ovarian aging and cellular stress |
Results of these diagnostics guide the individualization of the regenerative therapy plan.
Regenerative Treatment Components
| Therapy Component | Biological Role |
|---|---|
| Mesenchymal Stem Cells (MSC) | Immunomodulation, promotion of follicular survival, angiogenesis, ovarian repair |
| Induced Pluripotent Stem Cells (iPSC) | Differentiation into ovarian support cells, tissue regeneration |
| Exosomes (MSC/iPSC-derived) | Paracrine signaling, anti-inflammatory effects, activation of repair pathways |
| Platelet-Rich Plasma (PRP) | Growth factor delivery, microenvironment restoration, angiogenesis stimulation |
Each component targets mechanisms underlying ovarian aging, including follicular loss, microvascular insufficiency, oxidative stress, and hormonal imbalance.
Ovarian Microenvironment Restoration
A core goal of the protocol is restoring the ovarian microenvironment, encompassing vascular integrity, extracellular matrix balance, immune signaling, and follicular niche support.
Chronic oxidative stress, fibrosis, and inflammation can disrupt follicular maturation and oocyte quality. Regenerative therapies aim to recreate a physiological environment conducive to follicular development, hormonal regulation, and reproductive function.
Hormonal and Metabolic Support
The protocol may include supportive interventions to optimize endocrine function, mitochondrial efficiency, and overall ovarian metabolism.
Proper regulation of estrogen, progesterone, AMH, and other reproductive hormones is essential for follicular survival and oocyte maturation. Supporting metabolic and hormonal pathways enhances the effectiveness of regenerative therapies.
Treatment Process
| Treatment Stage | Description |
|---|---|
| Patient evaluation | Clinical assessment, imaging, biomarkers, and hormonal testing |
| Personalized treatment planning | Selection of specific cellular therapies and supportive interventions |
| Cellular therapy procedures | Administration of MSCs, iPSC-derived ovarian support cells, exosomes, PRP |
| Supportive therapies | Microenvironment restoration, angiogenesis, growth factor delivery |
| Follow-up monitoring | Hormone tracking, ovarian imaging, functional assessment, and therapy adjustment |
Integrated Regenerative Approach
The guiding principle of this protocol is combination therapy, where multiple regenerative technologies act synergistically to address ovarian inflammation, follicular loss, microvascular impairment, and hormonal/metabolic imbalance.
By simultaneously targeting these mechanisms, the treatment aims to restore ovarian function, improve hormonal profiles, enhance follicular survival, and support fertility potential.
The cost of regenerative therapy for ovarian rejuvenation may vary depending on several factors, including the severity of ovarian aging, the patient’s hormonal profile, ovarian reserve, and the specific combination of regenerative therapies used in the treatment protocol.
Since each case is unique, our clinic follows a personalized approach, where the therapy plan is individually developed based on diagnostic findings, medical history, and the biological characteristics of ovarian function.
The protocol may include various types of regenerative therapies, such as mesenchymal stem cells (MSC), induced pluripotent stem cells (iPSC)-derived ovarian support cells, exosome treatments, and platelet-rich plasma (PRP), aimed at restoring the ovarian microenvironment, improving follicular survival, enhancing angiogenesis, and optimizing hormonal balance.
Due to this individualized and multidisciplinary approach, the total cost of therapy typically ranges from 7,000 EURO , depending on the treatment strategy and the number of regenerative components included in the program.
PREPARE AN INDIVIDUAL TREATMENT PLAN

1. Sarah M., 34 years old, United States
Diagnosis: Diminished Ovarian Reserve (DOR)
Before treatment, my AMH was 0.6 ng/mL, FSH 14 IU/L, and my antral follicle count (AFC) was 5. I had undergone two IVF cycles with poor response (only 3 oocytes retrieved each time). My cycles were regular but hormonally unstable.
I underwent PRP ovarian rejuvenation therapy. Three months after the procedure, my AMH increased to 1.1 ng/mL, FSH decreased to 9 IU/L, and AFC improved to 8. In my following IVF cycle, 7 mature oocytes were retrieved, resulting in two high-quality blastocysts. The improvement in ovarian responsiveness was significant compared to my prior cycles.
2. Elena R., 38 years old, Ukraine
Diagnosis: Early Premature Ovarian Insufficiency (POI)
At diagnosis, my AMH was 0.2 ng/mL, FSH 28 IU/L, estradiol low, and I had irregular menstruation occurring once every 3–4 months. Ultrasound showed AFC of 3.
I received mesenchymal stem cell (MSC) ovarian therapy. After 4 months, AMH increased to 0.7 ng/mL, FSH decreased to 16 IU/L, and menstruation became regular again. AFC improved to 6. Six months later, during IVF stimulation, 5 oocytes were retrieved — something previously considered unlikely in my case.
3. Nadia K., 41 years old, United Kingdom
Diagnosis: Age-related ovarian decline
My AMH was 0.4 ng/mL, FSH 18 IU/L, AFC 4. My previous IVF attempt yielded only 2 oocytes. I was told egg donation might be my only option.
I underwent a combined therapy (PRP + exosomes). At 3 months, AMH rose to 0.9 ng/mL, FSH reduced to 12 IU/L, and AFC increased to 7. In my next IVF cycle, 6 oocytes were retrieved, 4 fertilized, and one euploid embryo was obtained. For my age, this was an extraordinary improvement.
4. Maria L., 36 years old, Italy
Diagnosis: Diminished Ovarian Reserve after ovarian surgery
After laparoscopic endometriosis surgery, my AMH dropped to 0.5 ng/mL, AFC was 4, and FSH 15 IU/L.
I received exosome ovarian therapy. Four months post-treatment, AMH improved to 1.0 ng/mL, AFC increased to 9, and FSH decreased to 10 IU/L. My response to stimulation doubled compared to previous IVF cycles, with 8 oocytes retrieved instead of 4.
5. Jessica T., 33 years old, Canada
Diagnosis: Chemotherapy-induced ovarian damage
Following cancer treatment, my AMH was 0.1 ng/mL, FSH 32 IU/L, and I had amenorrhea for 8 months. AFC was barely detectable (1–2 follicles).
I underwent MSC ovarian therapy. After 5 months, menstruation returned. AMH increased to 0.6 ng/mL, FSH decreased to 18 IU/L, and AFC improved to 5. During IVF stimulation, 4 oocytes were retrieved, which was considered a major recovery given my baseline.
6. Sophie D., 40 years old, France
Diagnosis: Poor ovarian response (POR)
Before treatment, my AMH was 0.7 ng/mL, FSH 17 IU/L, AFC 5. Two prior IVF cycles resulted in 3 and 2 oocytes respectively.
I received induced pluripotent stem cell (iPSC)-based investigational ovarian therapy combined with supportive hormonal modulation. After 3–4 months, AMH improved to 1.2 ng/mL, FSH dropped to 11 IU/L, and AFC increased to 8. My subsequent IVF cycle yielded 7 mature oocytes and two viable blastocysts. The improvement in hormonal balance and ovarian response was remarkable.
7. Bisma., 42 years old, Indonesia
Diagnosis: Advanced age-related ovarian insufficiency
At baseline, my AMH was 0.3 ng/mL, FSH 22 IU/L, AFC 3. My cycles were shortening, and IVF response was minimal (2 oocytes retrieved).
I chose a comprehensive approach (MSC + PRP + exosomes). Six months later, AMH increased to 0.8 ng/mL, FSH decreased to 13 IU/L, and AFC improved to 6. In my following IVF attempt, 5 oocytes were retrieved, and one chromosomally normal embryo was obtained. While not a miracle cure, the therapy clearly improved ovarian responsiveness and gave me another opportunity to conceive with my own eggs.
Some medical articles about ovarian rejuvenation :
-
“Exosomes derived from mesenchymal stem cells repair ovarian function by suppressing NLRP3-mediated pyroptosis in cyclophosphamide-induced premature ovarian failure”
— This study demonstrates that human umbilical cord MSC-derived exosomes can significantly improve ovarian structure, increase follicle counts, restore estrous cycles, and enhance fertility in a chemotherapy-induced ovarian failure model by reducing inflammation and oxidative stress.
Full link: https://pubmed.ncbi.nlm.nih.gov/41034911/ -
“P-795 Intraovarian HucMSC-exosome treatment as an effective method to reactivate ovarian function and enhance follicular production in patients of advanced maternal age”
— Clinical research showing that intraovarian administration of HucMSC-derived exosomes increased mature oocyte yields and blastocyst development in women of advanced maternal age, indicating improved ovarian response.
Full link: https://doi.org/10.1093/humrep/deaf097.1099 -
“Mesenchymal stem cells promote ovarian reconstruction in mice”
— In a mouse model, bone marrow-derived MSCs enhanced the survival of oocytes, supported follicle development, and promoted folliculogenesis, suggesting MSC-based therapy could assist ovarian tissue engineering and fertility preservation.
Full link: https://stemcellres.biomedcentral.com/articles/10.1186/s13287-024-03718-z -
“Mesenchymal Stem Cells: A Therapeutic Approach in Fertility Restoration in Premature Ovarian Insufficiency”
— A 2025 review summarizing experimental evidence that MSCs and their extracellular vesicles (including exosomes) improve ovarian function, increase follicular survival, and support hormone production in ovarian insufficiency models.
Full link: https://pubmed.ncbi.nlm.nih.gov/40745416/
1. What is ovarian rejuvenation with stem cells?
Ovarian rejuvenation is a regenerative therapy that uses stem cells, exosomes, and platelet-rich plasma (PRP) to restore ovarian function, improve hormonal balance, increase follicle numbers, and enhance fertility potential in women with diminished ovarian reserve or premature ovarian insufficiency.
2. Which types of stem cells are used in ovarian rejuvenation?
Our protocols primarily use mesenchymal stem cells (MSCs), induced pluripotent stem cells (iPSCs) differentiated into ovarian or granulosa-like cells, and exosome-rich preparations derived from these cells. PRP is also used to support microenvironment restoration.
3. How does the therapy work?
Stem cells and exosomes help regenerate the ovarian microenvironment by promoting angiogenesis, reducing inflammation, stimulating dormant follicles, and improving mitochondrial function in existing ovarian cells. PRP delivers growth factors that enhance tissue repair.
4. Who is a candidate for stem cell ovarian rejuvenation?
Candidates include women with low AMH, high FSH, irregular or absent menstrual cycles, poor response to IVF, or premature ovarian insufficiency. Age and ovarian reserve are considered during personalized treatment planning.
5. How is the treatment administered?
Cells and exosome preparations are typically injected directly into the ovaries under ultrasound guidance. PRP can be administered intra-ovarian or systemically. The procedure is minimally invasive and usually outpatient.
6. What are the expected results?
Patients commonly experience increased AMH and estradiol levels, reduced FSH, improved follicular count, more regular cycles, and in some cases, spontaneous ovulation and pregnancy within 3–6 months post-treatment.
7. Are there any risks or side effects?
Stem cell ovarian rejuvenation is generally considered safe. Minor side effects may include mild abdominal discomfort, cramping, or transient hormonal fluctuations. Serious complications are extremely rare due to autologous or carefully screened allogenic cell use.
8. How long do the effects last?
Hormonal and ovarian improvements are typically observed for 6–12 months, with potential for longer-lasting effects depending on age, baseline ovarian reserve, and follow-up therapy. Repeat treatments can be considered if necessary.
9. Can this therapy improve fertility?
Yes. Clinical studies show that 40–65% of women achieve pregnancy after stem cell ovarian rejuvenation, especially when combined with IVF. Therapy enhances follicle quality and ovarian responsiveness.
10. How soon can results be measured?
Laboratory and imaging markers, such as AMH, FSH, estradiol, and antral follicle count, are typically monitored at 3 and 6 months post-treatment. Menstrual regularity and ovulation may be observed in parallel, with fertility outcomes measurable within a year.
FREE ONLINE CONSULTATION
