
Stem cell therapy is one of the most promising areas of modern regenerative medicine. However, patients and even some physicians sometimes expect results too quickly, or conversely, anticipate unjustifiably delayed outcomes. To understand realistic timelines, it is important to consider the type of stem cells, their mechanism of action, the patient’s condition, and the nature of the disease.
How Stem Cells Work: Key Mechanisms
The result of therapy depends on what exactly the stem cells do after administration:
- Direct regeneration – differentiation of administered cells into cells of the lost tissue (less common, slower).
- Paracrine effect – secretion of growth factors, cytokines, and exosomes that stimulate the body’s own cells to recover (more common, faster).
- Immunomodulation – suppression of pathological inflammation and normalization of immune response, creating conditions for regeneration.
Factors Influencing the Time to See Results
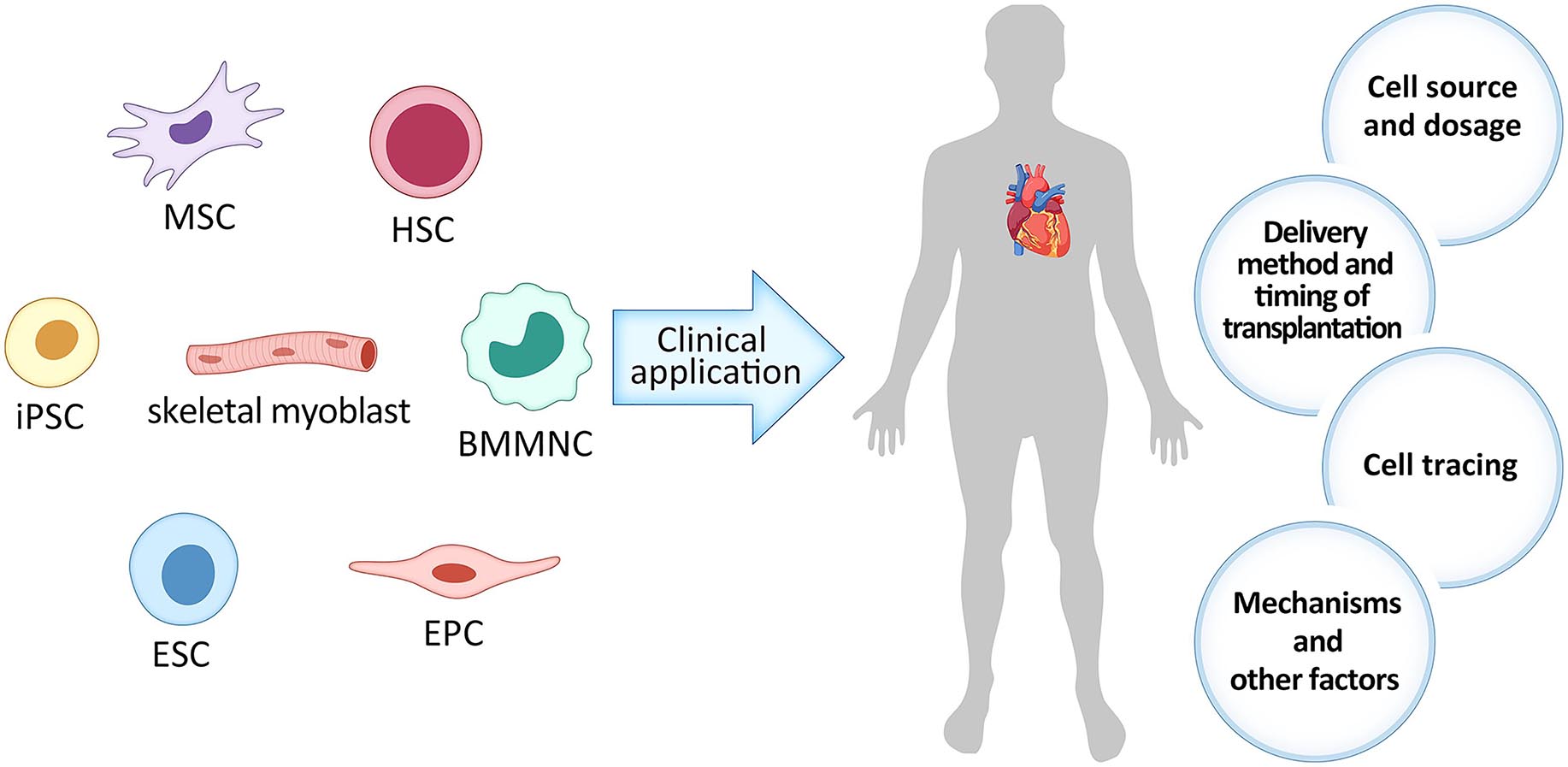
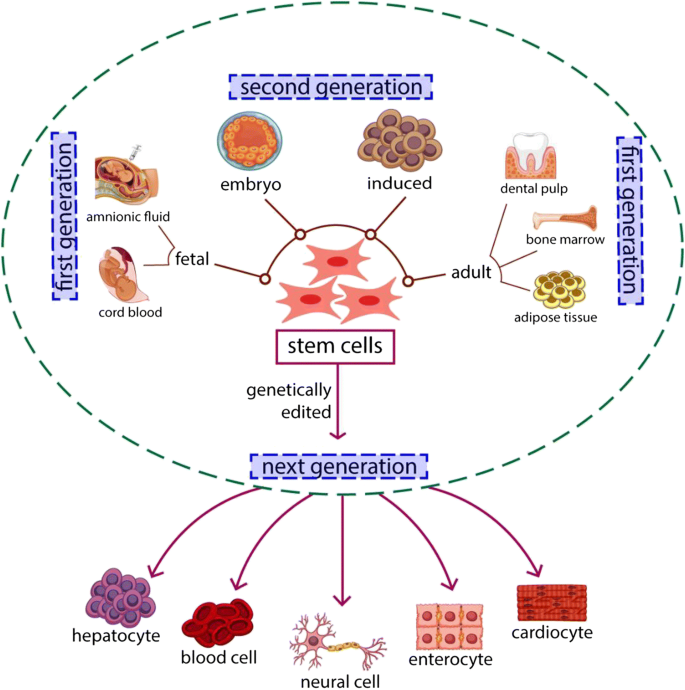
Type of Cells and Their Source
- Mesenchymal stromal cells (MSC) – effects often start with anti-inflammatory changes (2–6 weeks), with a regenerative peak at 3–6 months.
- Hematopoietic stem cells (HSC) – after transplantation, restoration of hematopoietic function takes 2–4 weeks, and immune stabilization takes months.
- Induced pluripotent stem cells (iPSC) – timing depends on the stage of differentiation; often delayed for months, averaging from 3 months.
- Exosomes and other extracellular vesicles – their action is often associated with triggering regeneration cascades, modulating inflammation, and improving cellular metabolism. Initial effects (reduced inflammation, improved skin condition, partial increase in energy) may be noticeable within 1–4 weeks, but structural changes (tissue regeneration, functional recovery) usually manifest within 1–3 months.
- Narrowly differentiated cells (e.g., chondrocytes, neuroblasts, myoblasts) – may integrate more slowly. Engraftment and functionality take time; first improvements are possible after 3 months, with a peak effect at 6–12 months.
- Mitochondrial therapy (transplantation of isolated mitochondria or stimulation of biogenesis) can produce a faster metabolic effect – sometimes within days or weeks, but a lasting functional result takes months.
Disease and Its Stage
- Acute injury (e.g., limb ischemia) – clinical effect may appear within days or weeks.
- Chronic degenerative diseases (osteoarthritis, neurodegeneration) – results develop slowly, usually over 3–12 months.
- Autoimmune diseases – improvement may occur after immune stabilization, which takes 3–4 months.
Individual Factors
- Age of the patient (younger → faster regeneration).
- Immune status.
- Comorbidities and use of medications (especially immunosuppressants or corticosteroids).
Typical Recovery Dynamics
| Period After Therapy | Biological Processes | Possible Clinical Changes |
| 0–2 weeks | Immunomodulation, reduced inflammation, cell adaptation | Reduction in pain, swelling, general improvement in well-being in some patients |
| 1–3 months | Paracrine stimulation of regeneration, activation of the body’s own progenitor cells | Improved organ/tissue function, symptom reduction |
| 3–6 months | Maturation of new cells, restoration of microcirculation, tissue remodeling | Maximum functional gain, stabilization of condition |
| 6–12 months | Long-term effects and maintenance of restored functions | Consolidation of results, sometimes further improvement |
Why There Is Not Always a Quick Result
- Prolonged phase of cell integration and maturation.
- Presence of irreversible tissue changes.
- Strong chronic inflammation or active autoimmune process.
- Insufficient cell dose or viability.
Stem Cell Path: From Administration to Clinical Effect
- 0–24 hours — adaptation and survival of cells
What happens: cells encounter a new environment; some die, some attach to tissues.
What may slow it down: low cell viability, high inflammation, poor blood supply.
How to accelerate: use fresh/high-quality cells, reduce systemic inflammation beforehand, improve microcirculation.
- 1–14 days — interaction with tissues and immunomodulation
What happens: cells secrete anti-inflammatory cytokines, begin paracrine effects on local cells.
What may slow it down: excessive immune response, autoimmune aggression.
How to accelerate: mild immunosuppression as indicated, use of exosomes or growth factors in parallel.
- 2–8 weeks — stimulation of regeneration and activation of own progenitor cells
What happens: new vessels form, local stem cells are activated, inflammation decreases.
What may slow it down: fibrosis, chronic infections, vitamin/mineral deficiencies.
How to accelerate: physiotherapy, correction of deficiencies (D, B12, magnesium), PRP or growth factors.
- 3–6 months — maturation and integration of new cells
What happens: administered and activated cells become mature tissue structures, functions are restored.
What may slow it down: tissue ischemia, recurrent inflammation, lack of stimulation (physical inactivity).
How to accelerate: physical therapy, rehabilitation, supportive therapy (angioprotectors, mitochondrial stimulators).
- 6–12 months — effect stabilization
What happens: consolidation of functional improvements, tissue adaptation to new conditions.
What may slow it down: disease recurrence, unaddressed risk factors.
How to accelerate/maintain: repeat therapy courses (if indicated), control of chronic diseases, healthy lifestyle.

PREPARE AN INDIVIDUAL TREATMENT PLAN
