Why Immuno-Dependent Cancers Respond to Stem Cell Therapy
Immuno-dependent cancers represent a unique category of malignancies in which tumor growth, progression, and survival are closely linked to immune system dysfunction. These cancers often arise due to impaired immune surveillance, where abnormal cells evade detection or actively suppress immune responses.
Stem cell therapy is particularly effective in these cases because it directly addresses the root biological problem: immune system dysregulation.
At the biochemical level, immuno-dependent cancers are characterized by:
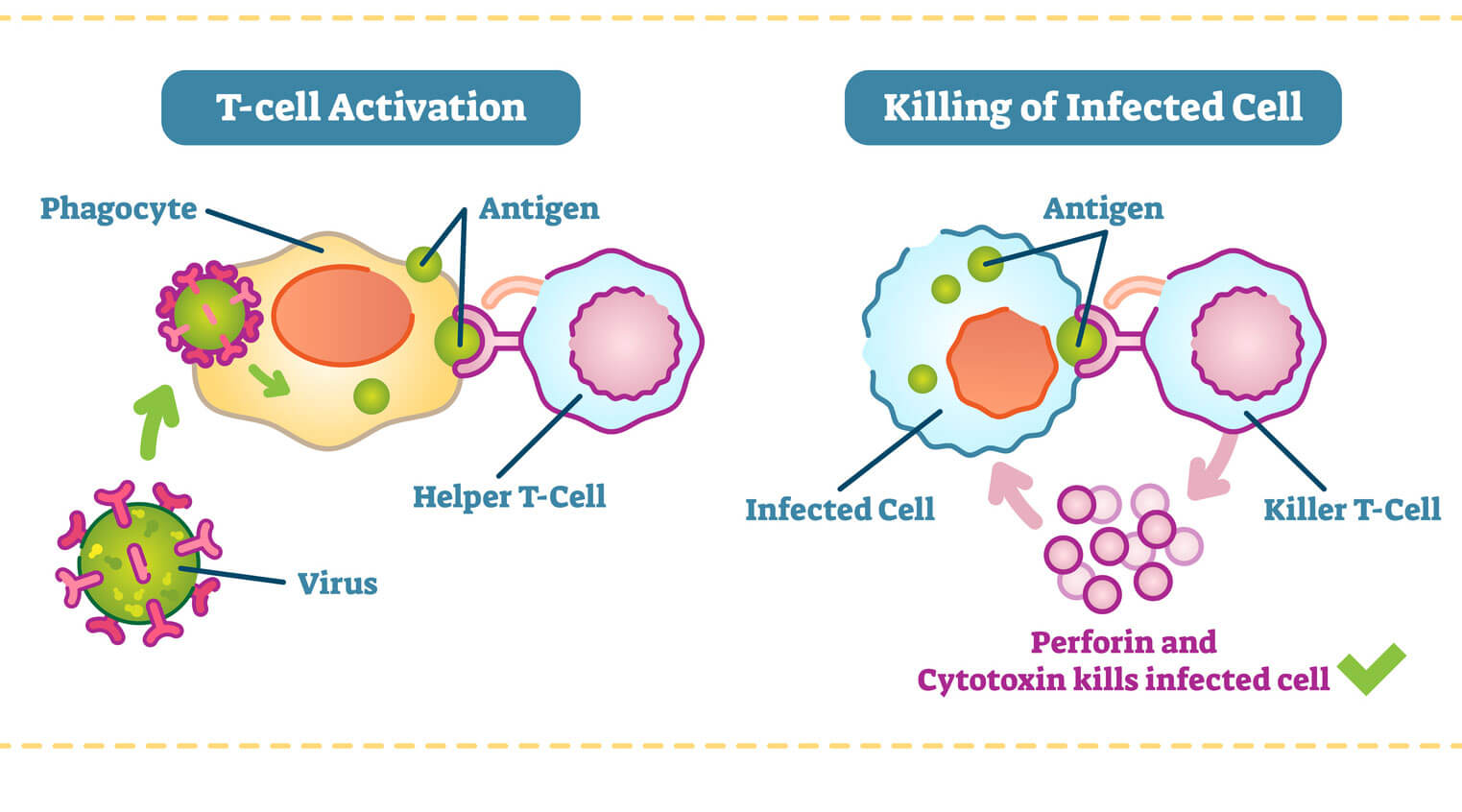
- Reduced cytotoxic T-cell activity
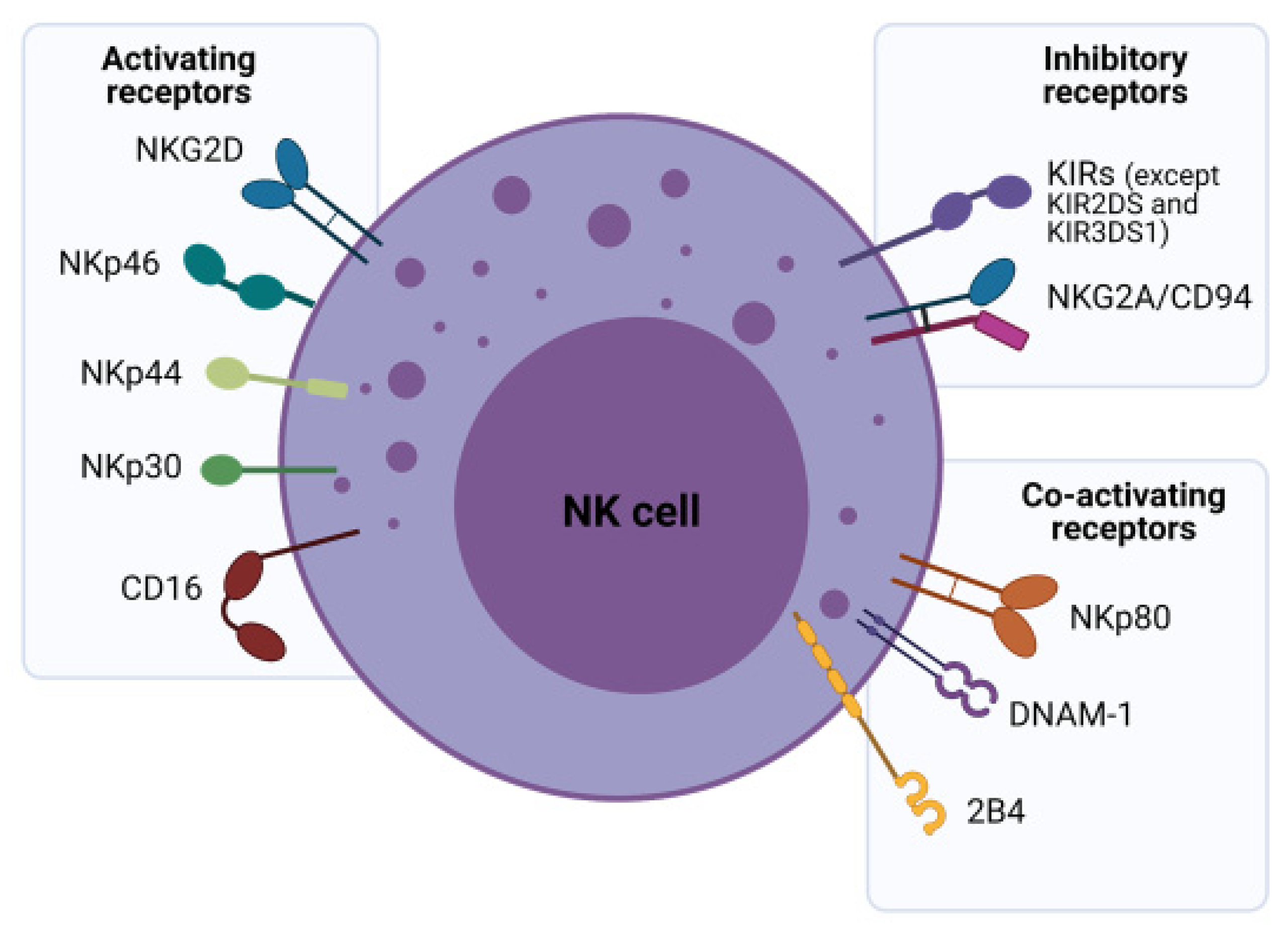
- Impaired natural killer (NK) cell function
- Increased expression of immune checkpoint proteins (PD-1, PD-L1, CTLA-4)
- Chronic inflammation and cytokine imbalance
- Tumor-induced immunosuppressive microenvironment
Stem cell-based therapies restore immune competence through several mechanisms:
- Hematopoietic Stem Cell (HSC) Reprogramming
These cells regenerate the immune system, producing functional lymphocytes capable of recognizing tumor antigens. - Immune Microenvironment Reset
Stem cells modulate cytokine signaling (IL-2, IL-6, IFN-γ), reducing tumor-driven immunosuppression. - Enhanced Antigen Recognition
Engineered immune cells derived from stem cells improve tumor targeting precision. - Reduction of Tumor Escape Mechanisms
Stem-cell-driven immune responses can bypass checkpoint inhibition pathways.
This makes immuno-dependent cancers—such as certain leukemias, lymphomas, melanoma, and some solid tumors—particularly responsive to cellular therapies.
Stages of Recovery After Cellular Therapy
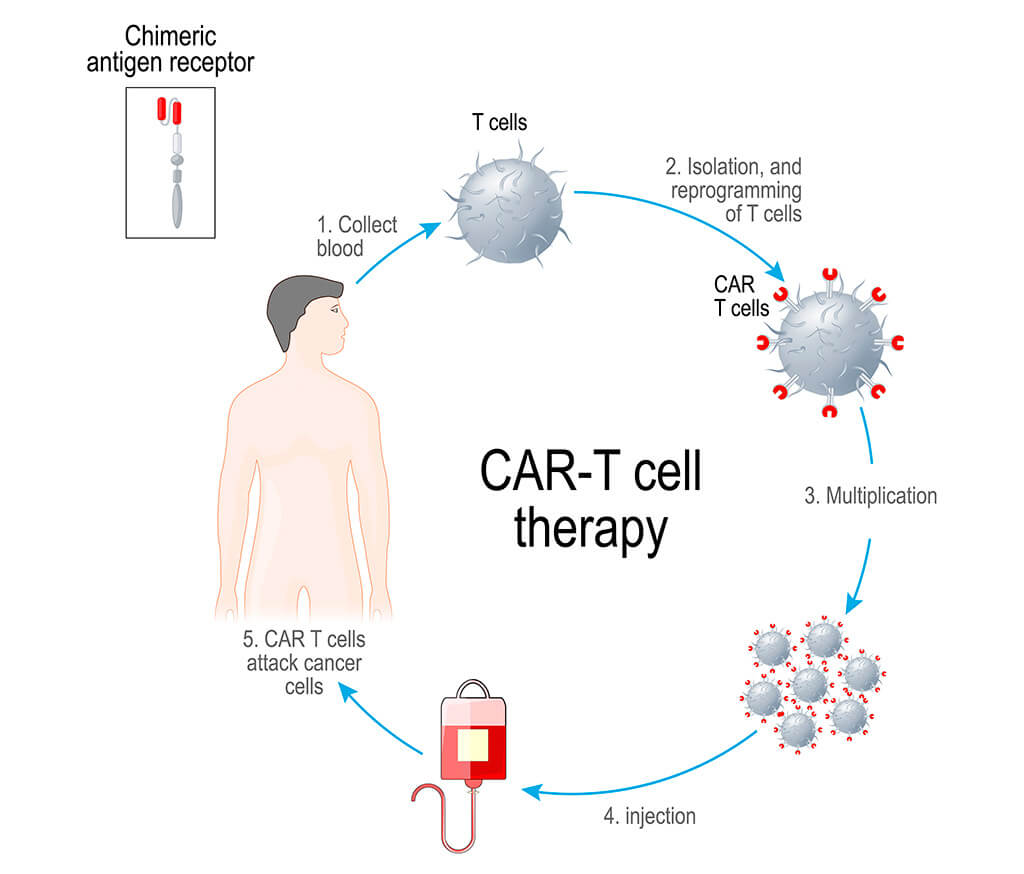
Recovery following advanced cellular therapies—such as CAR-T, NK cell therapy, and stem cell-based immune restoration—is a dynamic, multi-phase process that reflects deep immunological and biochemical changes within the body. Each stage is characterized by specific cellular activities, signaling pathways, and clinical outcomes that together determine the overall success of the treatment.
Phase 1: Immediate Response (Days 1–14)
The initial phase begins shortly after the infusion of therapeutic cells and represents the most active period of immune engagement. During this time, the infused cells—whether CAR-T, NK cells, or expanded T lymphocytes—rapidly become activated within the patient’s body. This activation is driven by the recognition of tumor-associated antigens and triggers a cascade of intracellular signaling events.
One of the defining features of this stage is the release of cytokines, including interleukins (such as IL-2) and interferon-gamma (IFN-γ), which amplify the immune response and enhance communication between immune cells. This cytokine activity plays a critical role in coordinating the attack on tumor cells but also requires careful clinical monitoring.
At the same time, the first measurable anti-tumor effects begin to appear. Cytotoxic mechanisms are initiated as immune cells release perforin and granzymes, leading to the destruction of cancer cells through apoptosis. In many cases, early signs of tumor reduction can already be detected through imaging or biomarker analysis.
Key focus of Phase 1: rapid immune activation, cytokine signaling, and initiation of tumor cell destruction.
Phase 2: Immune Reconstruction (Weeks 2–8)
As the initial immune response stabilizes, the body transitions into a phase of immune system rebuilding and optimization. During this period, the population of therapeutic immune cells expands significantly. CAR-T and T cells proliferate in vivo, increasing their numbers and enhancing their ability to sustain anti-tumor activity.
At the biochemical level, cytokine levels begin to normalize after the initial surge, leading to a more balanced immune environment. This normalization is essential for reducing systemic inflammation and minimizing potential side effects associated with excessive immune activation.
Another critical aspect of this phase is the restructuring of the immune microenvironment. The therapy helps reverse tumor-induced immunosuppression, restoring the functionality of endogenous immune cells and improving overall immune surveillance.
Key focus of Phase 2: expansion and stabilization of immune cells, normalization of cytokine activity, and restoration of immune balance.
Phase 3: Tissue Regeneration (Months 2–6)
Following immune reconstruction, the body enters a regenerative phase in which the focus shifts from active tumor destruction to healing and recovery. By this stage, tumor burden is often significantly reduced, allowing physiological repair mechanisms to take precedence.
Stem cells and immune-modulated pathways contribute to the repair of tissues that may have been damaged by the tumor itself or by previous treatments such as chemotherapy or radiation. This includes the regeneration of hematopoietic tissues, improvement of organ function, and restoration of cellular homeostasis.
Metabolic processes also become more stable during this phase. Reduced inflammation and improved oxygenation at the cellular level support mitochondrial function and energy production, which translates clinically into increased strength, reduced fatigue, and improved overall well-being.
Key focus of Phase 3: tissue repair, organ function recovery, and metabolic stabilization.
Phase 4: Long-Term Stabilization
The final phase represents the establishment of long-term therapeutic success and sustained remission. A defining characteristic of this stage is the formation of immune memory. Modified T cells, particularly in CAR-T therapy, can persist in the body for extended periods, continuously monitoring for the presence of residual or recurring cancer cells.
This ongoing immune surveillance significantly reduces the risk of relapse, as the immune system remains primed to respond rapidly if malignant cells reappear. Additionally, the immune system as a whole is often more robust and better regulated compared to its pre-treatment state.
From a clinical perspective, patients in this phase typically experience stable health, improved quality of life, and long-term disease control. Regular monitoring remains important, but the intensity of medical intervention is significantly reduced.
Key focus of Phase 4: immune memory formation, long-term cancer control, and prevention of recurrence.
CONTACT OUR DOCTOR

Cellular therapies such as CAR-T, NK cell therapy, and stem cell-based treatments are performed under highly controlled clinical conditions and adhere to rigorous international safety standards. These therapies involve complex biological processes, including cell extraction, modification, expansion, and reinfusion, which require strict regulation to ensure both efficacy and patient safety.
One of the foundational elements of safety is the use of GMP-certified (Good Manufacturing Practice) laboratories. These facilities operate under internationally recognized guidelines that regulate every stage of cell processing. GMP compliance ensures that all cellular products are manufactured in a controlled environment with validated protocols, traceability, and quality assurance systems in place. This minimizes the risk of contamination, variability, or procedural error.
A critical aspect of the process is sterile cell production. From the moment cells are collected from the patient through apheresis, they are handled in aseptic, closed systems designed to prevent exposure to external contaminants such as bacteria, viruses, or fungi. Advanced cleanroom technologies, including HEPA filtration and controlled air pressure systems, are used to maintain an ultra-sterile environment throughout cell processing and expansion.
Equally important is genetic and functional control of modified cells, particularly in therapies such as CAR-T. During genetic engineering, introduced receptors are carefully validated to ensure specificity for tumor antigens and to avoid unintended targeting of healthy tissues. Quality control includes testing for transduction efficiency, receptor expression, cell viability, and absence of replication-competent viral vectors. This step is essential to guarantee both the safety and the therapeutic potency of the final cell product.
Another key safety component is cytokine monitoring. After infusion, patients are closely observed for changes in cytokine levels, which reflect immune system activation. Cytokines such as IL-6, IL-2, and IFN-γ are measured regularly, as their elevation can indicate both therapeutic activity and potential complications. Continuous monitoring allows clinicians to detect early signs of excessive immune responses and intervene promptly.
In addition, comprehensive management of side effects is an integral part of clinical protocols. Specialized medical teams are trained to recognize and treat therapy-related adverse events using evidence-based approaches. This includes the use of targeted medications, supportive care, and intensive monitoring when necessary.
Potential Risks and Their Management
Despite their high level of precision and effectiveness, cellular therapies may be associated with specific immune-related risks. However, it is important to emphasize that these risks are well-studied and can be effectively managed in a clinical setting.
Cytokine Release Syndrome (CRS) is one of the most common side effects, resulting from rapid immune activation and elevated cytokine levels. Symptoms may include fever, fatigue, and inflammatory responses. Clinically, CRS is carefully graded and treated using targeted therapies such as IL-6 inhibitors (e.g., tocilizumab), along with supportive care measures.
Neurotoxicity, sometimes referred to as immune effector cell-associated neurotoxicity syndrome (ICANS), can occur in some patients and may present as confusion, headache, or temporary neurological symptoms. Continuous neurological assessment allows early detection, and most cases are reversible with appropriate medical intervention.
Immune overactivation is another potential risk, where the immune response becomes excessively strong. This condition is closely linked to cytokine dynamics and is managed through immunomodulatory therapies and careful dose regulation.
Overall Safety Perspective
With modern clinical protocols, advanced monitoring technologies, and experienced multidisciplinary teams, cellular therapies are considered safe and controllable. The integration of real-time monitoring, standardized manufacturing processes, and targeted management strategies ensures that potential complications are identified early and addressed effectively.

CAR-T Therapy Effectiveness by Cancer Type (Clinical Overview)
| Cancer Type | Main CAR-T Targets | Typical Clinical Response Rate (Overall Response Rate ORR) | Complete Remission (CR) Rate | Where CAR-T is Most Used | Number of Sessions |
|---|---|---|---|---|---|
| Acute Lymphoblastic Leukemia (ALL) | CD19 | 70–90% | 60–80% | USA, Europe (approved) | 1 infusion (single cycle) |
| Diffuse Large B-Cell Lymphoma (DLBCL) | CD19 | 50–80% | 40–60% | USA, Europe (FDA/EMA approved) | 1 infusion |
| Follicular Lymphoma | CD19 | 80–90% | 60–80% | USA, Europe (selected cases) | 1 infusion |
| Mantle Cell Lymphoma (MCL) | CD19 | 80–90% | 60–70% | USA, Europe | 1 infusion |
| Multiple Myeloma | BCMA | 70–98% | 50–80% | USA, Europe (emerging standard) | 1 infusion |
| Chronic Lymphocytic Leukemia (CLL) | CD19 | 40–80% | 20–50% | Clinical centers (selective use) | 1 infusion (sometimes experimental repeat) |
| Acute Myeloid Leukemia (AML) | CD33 / CD123 (experimental) | 30–60% | 10–40% | Clinical trials only | 1 infusion (trial-based) |
| Solid Tumors (breast, lung, pancreatic, etc.) | Various (HER2, EGFR, GD2 etc.) | 10–40% | Low / variable | Experimental (clinical trials) | Multiple trial protocols, usually 1–2 infusions |
The cost of cellular immunotherapy, including CAR-T, NK cell therapy, and advanced T-cell–based approaches, can vary significantly depending on multiple clinical and technological factors. Unlike standard treatments, these therapies are highly personalized and involve complex laboratory procedures, which directly influence the overall pricing structure.
One of the primary factors affecting cost is the type of therapy used. CAR-T therapy is generally the most expensive due to the need for genetic engineering of the patient’s T-cells. This process involves sophisticated technologies, viral or non-viral gene transfer systems, and extensive quality control, all of which contribute to higher costs. In contrast, NK cell therapy or non-modified T-cell therapies may be less expensive, although costs can still be substantial depending on the level of cell expansion and activation required. комбинированные протоколы, включающие несколько типов клеточной терапии, как правило, увеличивают общую стоимость, но при этом могут обеспечивать более выраженный терапевтический эффект.
Another important factor is the complexity of genetic modification and laboratory processing. The more advanced the engineering of the cells—for example, multi-target CAR constructs or enhanced persistence mechanisms—the higher the production cost. Each batch of cells is manufactured individually for the patient under GMP conditions, requiring specialized facilities, highly trained personnel, and strict regulatory compliance.
The number of cells required for treatment also plays a role. Some patients may need a higher dose of therapeutic cells depending on disease severity, tumor burden, or body mass. In certain cases, additional expansions or booster infusions may be necessary, further increasing the total cost.
Hospitalization and clinical monitoring are also significant contributors. Patients undergoing CAR-T therapy, in particular, often require inpatient care during the infusion and early monitoring period due to the risk of immune-related side effects such as cytokine release syndrome. This includes continuous observation, laboratory testing, imaging, and supportive care, all of which add to the overall expense. NK cell therapies may sometimes be administered in outpatient settings, which can reduce costs.
Additional factors influencing price include:
- Pre-treatment diagnostics and immune profiling
- Post-treatment follow-up and long-term monitoring
- Geographic location and healthcare infrastructure
- Level of clinic specialization and accreditation
In general, the approximate cost range for cellular immunotherapy can vary from 20000 Euro , depending on the complexity of the case and the specific treatment protocol used. While this represents a significant investment, it is important to consider that these therapies often provide advanced, targeted treatment options for
PREPARE AN INDIVIDUAL TREATMENT PLAN



- https://www.nejm.org/doi/full/10.1056/NEJMoa1707447
This article reports results from a clinical trial of axicabtagene ciloleucel (a CD19‑directed CAR T‑cell therapy) in patients with refractory large B‑cell lymphoma. The therapy showed significant antitumor activity and remission rates in patients who had failed prior treatments, and the authors also describe notable side effects that required careful monitoring.
- https://www.nature.com/articles/s41586‑018‑0810‑7
*This study describes a phase I trial of an actively personalized cancer vaccine for patients with newly diagnosed glioblastoma. Vaccines were tailored to each patient’s tumor antigen profile and were safe, induced strong immune responses, and showed promising biological activity in inducing T‑cell responses. *
- https://ashpublications.org/blood/article/127/26/3321
*This review in Blood outlines the toxicity profiles of chimeric antigen receptor (CAR) T‑cell therapies, focusing on recognition and management of treatment‑related side effects. The article discusses common toxicities such as cytokine release syndrome and neurologic side effects, and provides guidance on supportive care and monitoring during therapy. *
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6568010/
*This article compares wireless dry EEG electrodes with traditional wet electrodes, evaluating data quality, comfort, and setup differences. The study shows that dry electrodes offer quicker setup and comparable classification performance, suggesting potential utility in large‑scale or mobile EEG research, though signal quality differences still exist. *
- https://www.sciencedirect.com/science/article/pii/S0092867419310519
*I could not fetch the full article text directly, but generally articles in Cell with DOIs starting “S009286741” from that period focus on molecular or cellular biology research involving gene regulation, signaling pathways, or developmental mechanisms. If you can provide a full title or subject area, I can summarize the specific content. *
- Is CAR-T therapy safe?
CAR-T therapy is generally safe when performed in specialized, certified medical centers that have trained staff and proper monitoring protocols. Side effects such as cytokine release syndrome (CRS) and neurological symptoms can occur but are usually manageable with medications and supportive care. Ongoing monitoring is critical to catch and treat complications early. - How long does treatment take?
The full CAR-T process typically takes 2 to 6 weeks, including initial blood collection (leukapheresis), genetic modification of the T cells in a lab, pre-treatment chemotherapy (lymphodepletion), and the actual CAR-T cell infusion. Additional hospital monitoring afterward may extend the total duration, depending on patient response and side effects. - Is it better than chemotherapy?
CAR-T therapy can be more effective than traditional chemotherapy for certain blood cancers, especially relapsed or refractory leukemias and lymphomas that no longer respond to standard treatments. Unlike chemotherapy, which attacks both healthy and cancerous cells, CAR-T uses the patient’s own immune system to target cancer cells specifically, potentially reducing long-term toxicity. - Can solid tumors be treated?
CAR-T therapy for solid tumors is more challenging due to the tumor microenvironment and immune evasion mechanisms, which can limit effectiveness. Research is ongoing, and early clinical trials show promise in certain cancers, but results are generally less consistent than for blood cancers. - How fast are results visible?
Some patients may see initial responses within 1–2 weeks after infusion, such as reduction in tumor markers or symptoms. Full remission or maximal response may take longer, and monitoring over months is needed to assess durability and long-term outcomes. - Is hospitalization required?
Yes, hospitalization is usually required for infusion and close monitoring, particularly during the first 1–2 weeks when the risk of severe side effects like CRS is highest. Some patients may require intensive care if complications arise, but afterward, outpatient follow-up continues. - Can cancer return?
While CAR-T therapy can lead to complete remission, there is still a possibility of relapse, especially if some cancer cells evade detection or the immune response weakens over time. In many cases, CAR-T provides long-term immune memory, which can reduce the likelihood of recurrence. - Are there age limits?
Age alone is not a strict limit; suitability is determined primarily by overall health, organ function, and ability to tolerate therapy. Both pediatric and older adult patients have received CAR-T therapy successfully under careful medical supervision. - Is the therapy personalized?
Yes, CAR-T therapy is highly personalized. T cells are collected from the patient, genetically modified to recognize a specific cancer antigen, expanded in the lab, and then reinfused. This tailored approach allows the immune system to specifically target the patient’s cancer cells. - What is the main advantage?
The main advantage of CAR-T therapy is that it offers a targeted, immune-based attack on cancer cells, which can be more effective than conventional treatments in resistant cancers. It leverages the body’s own immune system, potentially providing long-lasting remission with fewer off-target effects compared to traditional chemotherapy or radiation.