Chronic prostatitis is one of the most challenging and persistent urological conditions affecting men worldwide. It is estimated that 8–15% of men experience symptoms of chronic prostatitis or chronic pelvic pain syndrome (CPPS) during their lifetime. The disease often becomes a long-term health issue, significantly affecting quality of life, sexual function, urinary comfort, and psychological well-being.
Traditional treatments such as antibiotics, anti-inflammatory drugs, alpha-blockers, and physiotherapy are commonly prescribed. However, these therapies frequently provide only temporary symptom relief. Many patients continue to suffer from recurrent pelvic pain, urinary dysfunction, and inflammation even after months or years of treatment.
In recent years, regenerative medicine and stem cell therapy have emerged as promising approaches for treating chronic prostatitis. These innovative treatments aim not only to control symptoms but also to restore prostate tissue, regulate immune responses, improve blood circulation, and normalize hormonal balance.
Modern regenerative protocols often include stem cells, exosomes, platelet-rich plasma (PRP), and other biobank-derived biological products. By targeting the underlying causes of chronic inflammation and tissue damage, these therapies may offer new hope for patients who have not responded to conventional treatments.
This article provides a detailed overview of chronic prostatitis, its causes, age-related factors, and the role of stem cells and advanced biological therapies in restoring prostate function.

What Is Chronic Prostatitis?
Chronic prostatitis refers to persistent inflammation or dysfunction of the prostate gland lasting longer than three months. The disease can manifest through a wide range of symptoms, including:
- Pelvic or perineal pain
- Pain during ejaculation
- Urinary urgency or frequency
- Weak urinary stream
- Erectile dysfunction
- Chronic fatigue and discomfort
Unlike acute infections, chronic prostatitis often involves complex interactions between immune, hormonal, vascular, and neurological systems.
Main Clinical Types
Chronic prostatitis is usually classified into four categories:
- Chronic bacterial prostatitis
- Chronic pelvic pain syndrome (inflammatory)
- Chronic pelvic pain syndrome (non-inflammatory)
- Asymptomatic inflammatory prostatitis
The majority of patients fall into the chronic pelvic pain syndrome category, where no clear bacterial infection can be identified.
Major Causes of Chronic Prostatitis
Chronic prostatitis is considered a multifactorial disease, meaning that several mechanisms contribute simultaneously to its development.
Persistent Low-Grade Infection
Even when bacterial cultures appear negative, hidden microbial colonies may remain inside prostate ducts. Bacterial biofilms can protect pathogens from antibiotics, leading to persistent inflammation.
Immune Dysregulation
Many patients show elevated levels of inflammatory cytokines in prostatic fluid, including:
- IL-6
- TNF-α
- IL-1β
These molecules sustain inflammation and contribute to tissue damage.
Microcirculation Impairment
Reduced blood flow in prostate tissue leads to oxygen deficiency and metabolic stress, which slows healing and promotes inflammatory reactions.
Oxidative Stress
Chronic inflammation generates reactive oxygen species (ROS) that damage cellular structures, DNA, and proteins. Over time, oxidative stress can lead to tissue degeneration and fibrosis.
Hormonal Imbalance
Androgen signaling plays an essential role in prostate health. Reduced testosterone or impaired androgen receptor activity may contribute to inflammation and decreased regenerative capacity.
Pelvic Floor Dysfunction
Muscle tension in the pelvic floor may compress prostate tissue, impair lymphatic drainage, and worsen inflammation.
Chronic prostatitis can affect men of all ages, but its underlying mechanisms may differ depending on age.
Young Men (20–35 years)
In younger patients, chronic prostatitis is often associated with:
- Post-infectious inflammation
- Pelvic muscle tension
- Stress-related immune activation
- Lifestyle factors such as prolonged sitting
Prostate tissue in this age group has high regenerative potential, making regenerative therapies particularly effective.
Middle-Aged Men (35–50 years)
In this group, chronic prostatitis often overlaps with:
- Early vascular dysfunction
- Declining testosterone levels
- Metabolic syndrome
Patients may experience both urinary symptoms and sexual dysfunction.
Older Men (50+ years)
In older individuals, prostatitis may coexist with:
- Benign prostatic hyperplasia (BPH)
- Reduced hormonal activity
- Chronic systemic inflammation
Regenerative treatments for this group must address both inflammation and age-related tissue degeneration.
Why Conventional Treatments Often Fail
Standard therapies focus primarily on symptom control.
Common treatments include:
- Antibiotics
- Anti-inflammatory medications
- Alpha-blockers
- Pain management
- Pelvic physiotherapy
While these therapies may reduce symptoms temporarily, they rarely address the core biological mechanisms, such as:
- Chronic immune activation
- Tissue damage
- Microvascular dysfunction
- Hormonal imbalance
As a result, many patients experience recurrent symptoms.
FREE MEDICAL EVALUATION

Regenerative Medicine and Stem Cell Therapy
Stem cell therapy aims to restore normal tissue function by stimulating regeneration and regulating immune activity.
Key Biological Effects of Stem Cells
Anti-Inflammatory Action
Stem cells reduce the activity of inflammatory pathways and decrease cytokine production.
Tissue Regeneration
They stimulate regeneration of damaged epithelial and stromal prostate cells.
Microvascular Repair
Growth factors released by stem cells improve blood circulation within prostate tissue.
Immune Modulation
Stem cells regulate immune responses and prevent chronic inflammatory reactions.
Anti-Fibrotic Effects
They inhibit fibrotic processes and support healthy tissue remodeling.
An increasing number of patients with chronic prostatitis are experiencing meaningful improvements through regenerative medicine because these therapies target the underlying biological mechanisms of the disease rather than only suppressing symptoms. Chronic prostatitis is often associated with persistent inflammation, impaired microcirculation, oxidative stress, and degeneration of prostate tissue—factors that conventional treatments do not fully address. Regenerative approaches such as stem cells, exosomes, and other biobank-derived biological products work at the cellular level to reduce inflammatory signaling, promote tissue repair, stimulate angiogenesis, and restore the functional microenvironment of the prostate. In addition, these therapies can modulate immune responses and support hormonal balance, which are critical for long-term prostate health. By addressing multiple pathological pathways simultaneously, regenerative medicine offers a more comprehensive strategy for improving urinary function, reducing pelvic pain, and enhancing overall quality of life in patients with chronic prostatitis.
Types of Stem Cells Used in Chronic Prostatitis Treatment
Modern regenerative protocols may involve different cell types depending on clinical goals
Mesenchymal Stem Cells (MSC)
Mesenchymal stem cells are the most widely used regenerative cells in urology.
Sources include:
- Bone marrow
- Adipose tissue
- Umbilical cord
- Wharton’s Jelly
Mechanism of Action
Mesenchymal stem cells are considered one of the key therapeutic components due to their strong immunomodulatory and anti-inflammatory properties. After administration, MSCs release a wide range of bioactive molecules such as interleukin-10 (IL-10), transforming growth factor-β (TGF-β), and prostaglandin E2, which help suppress chronic inflammatory signaling and reduce activation of immune cells within prostate tissue. In addition, MSCs secrete growth factors including VEGF, HGF, and IGF-1 that stimulate angiogenesis, improve microcirculation, and support regeneration of epithelial and stromal prostate cells
MSC therapy works primarily through paracrine signaling, meaning that cells release bioactive molecules that influence surrounding tissue.
Key effects include:
- Reduction of inflammatory cytokines
- Stimulation of angiogenesis
- Improvement of tissue repair
- Modulation of immune activity
Effectiveness
Clinical observations suggest:
- 50–55% reduction in pelvic pain symptoms
- 30–50% improvement in urinary function
- Reduction in inflammatory markers within 2–3 months
Exosome Therapy
Exosomes are nano-sized vesicles released by stem cells.
They contain:
- Growth factors
- microRNA
- Anti-inflammatory proteins
Benefits
Exosomes can:
- Reduce inflammation
- Improve cell communication
- Promote tissue repair
- Protect prostate cells from oxidative stress
Exosomes, which are nano-vesicles secreted by stem cells, play a crucial role in intercellular communication. They contain microRNAs, proteins, and signaling molecules capable of regulating gene expression in damaged tissues, reducing oxidative stress, enhancing mitochondrial function, and promoting repair of prostate cells without the need for direct cell engraftment.
Clinical Results
Studies suggest that exosome therapy may lead to:
- 40–60% symptom improvement
- Faster recovery compared to standard therapy
Platelet-Rich Plasma (PRP)
PRP therapy uses the patient’s own blood plasma enriched with growth factors.
Key components include:
- PDGF
- VEGF
- TGF-β
- IGF
Mechanism
Platelet-rich plasma (PRP) contributes primarily through its high concentration of regenerative growth factors such as PDGF, TGF-β, VEGF, and EGF. These factors activate local progenitor cells, stimulate tissue remodeling, and accelerate healing processes while also improving vascularization of the prostate gland.
PRP stimulates:
- Tissue regeneration
- Blood vessel formation
- Cellular repair processes
Effectiveness
PRP therapy may lead to:
- 30–35% improvement in symptoms
- Reduced inflammation within 4–6 weeks
Induced Pluripotent Stem Cells (iPSC)
Induced pluripotent stem cells represent an advanced regenerative approach.
These cells are generated by reprogramming adult cells into a pluripotent state.
Potential Benefits
Induced pluripotent stem cell–derived progenitor cells represent an advanced regenerative strategy, as they can potentially differentiate into specialized cell types capable of replacing damaged glandular or stromal structures. At the biochemical level, these combined therapies influence key pathways involved in chronic prostatitis, including reduction of pro-inflammatory cytokines (IL-6, TNF-α), modulation of immune cell activity, improvement of nitric oxide–mediated microcirculation, activation of anti-oxidative mechanisms, and stimulation of extracellular matrix remodeling. Together, these processes help restore the prostate’s functional microenvironment, reduce chronic inflammation, and promote long-term regeneration of prostate tissue.
iPSC-derived cells may:
- Replace damaged prostate cells
- Restore glandular structure
- Improve long-term tissue regeneration
Expected Outcomes
Early studies suggest:
- Up to 80% functional tissue recovery in experimental models
Biobank-Derived Biological Products
Modern regenerative medicine often utilizes biobank cultures of therapeutic cells.
Advantages include:
- Standardized quality
- High viability
- Reduced treatment preparation time
Common products include:
- Cryopreserved MSC cultures
- Exosome concentrates
- Immune-regulating cell preparations
Our treatment strategy for chronic prostatitis is based on a comprehensive regenerative approach that combines several advanced biological therapies rather than relying on a single intervention. Chronic prostatitis is a multifactorial condition involving persistent inflammation, impaired microcirculation, immune imbalance, and disruption of the prostate microenvironment. Therefore, our protocol integrates mesenchymal stem cells (MSCs), stem cell–derived exosomes, and induced progenitor cells, each targeting different biological mechanisms of the disease. Mesenchymal stem cells provide strong immunomodulatory and anti-inflammatory effects, helping to suppress pro-inflammatory cytokines such as IL-6 and TNF-α while stimulating tissue repair and angiogenesis. At the same time, exosomes derived from regenerative cell cultures deliver microRNAs, proteins, and signaling molecules that enhance cellular communication, reduce oxidative stress, and support the recovery of damaged prostate cells.
Another important component of our approach is the correction of the prostate niche environment, which plays a crucial role in long-term recovery. Chronic prostatitis often leads to disruption of the local cellular microenvironment, including changes in stromal support cells, extracellular matrix structure, vascular supply, and immune regulation. Our therapeutic protocol focuses on restoring these conditions through regenerative signaling pathways that promote microvascular regeneration, reduce fibrosis, and stimulate the activity of endogenous repair mechanisms. Induced progenitor cells and biologically active growth factors further support the regeneration of epithelial and stromal structures within the prostate gland, helping to restore normal glandular function.
In addition to cellular therapy, we place significant emphasis on hormonal and metabolic correction, particularly the optimization of androgen signaling. Balanced androgen receptor activity is essential for prostate tissue regeneration and immune stability. Through the use of biologically active biobank products and supportive therapies aimed at improving androgen metabolism and receptor sensitivity, our approach seeks to normalize hormonal regulation within the prostate microenvironment. By combining regenerative cellular therapy, microenvironment restoration, and hormonal balance, this integrated protocol aims to achieve more sustainable improvements in prostate function, reduce chronic inflammation, and support long-term recovery for patients with chronic prostatitis.
Correction of the Prostate Microenvironment, why it’s important?
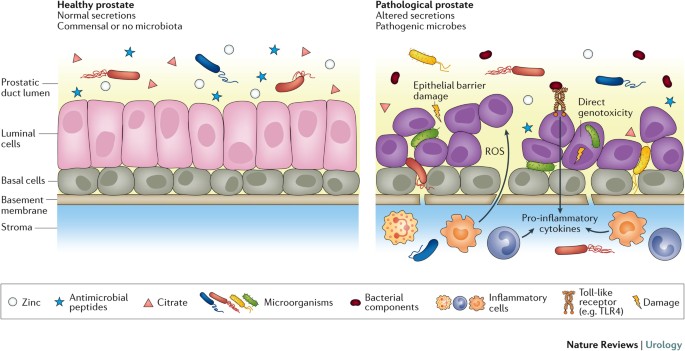
The prostate microenvironment refers to the complex biological environment surrounding prostate cells, including stromal cells, immune cells, blood vessels, nerve endings, extracellular matrix, and the network of signaling molecules that regulate tissue function. This microenvironment plays a crucial role in maintaining the normal structure and activity of the prostate gland. In chronic prostatitis, the prostate microenvironment becomes disrupted due to persistent inflammation, impaired microcirculation, oxidative stress, and immune imbalance. These changes lead to tissue irritation, fibrosis, and reduced regenerative capacity of prostate cells. As a result, even when infections are controlled or symptoms are temporarily relieved, the underlying inflammatory environment may continue to drive disease progression. Restoring a healthy prostate microenvironment is therefore essential for effective long-term treatment. Regenerative therapies such as stem cells, exosomes, and growth factor–based treatments aim to normalize this environment by reducing inflammatory cytokines, improving blood supply, regulating immune responses, and stimulating tissue repair. By correcting the cellular and biochemical conditions within the prostate, these therapies may help restore normal glandular function and reduce the recurrence of chronic prostatitis symptoms.
Successful treatment requires restoration of the prostate niche environment.
Key goals include:
Reducing Chronic Inflammation
Stem cells regulate immune responses and suppress inflammatory cytokines.
Improving Microcirculation
Growth factors stimulate new blood vessel formation.
Decreasing Oxidative Stress
Antioxidant pathways are activated to protect prostate tissue.
Supporting Tissue Regeneration
Regenerative signaling pathways stimulate new cell formation.
Hormonal Support and Androgen Restoration
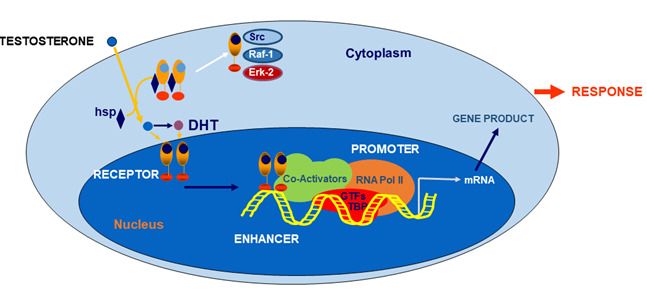
Androgen receptor (AR)–expressing cells play an essential role in maintaining normal prostate function and are an important factor in the treatment and recovery process of chronic prostatitis. Androgens such as testosterone and dihydrotestosterone (DHT) regulate the activity of prostate epithelial and stromal cells through androgen receptors, influencing cellular metabolism, immune regulation, and tissue regeneration. In chronic prostatitis, persistent inflammation, oxidative stress, and hormonal imbalance can disrupt androgen receptor signaling, leading to impaired prostate cell function, reduced secretory activity, and slower tissue repair. Restoration of proper AR signaling is therefore an important therapeutic target. Regenerative approaches, including stem cell therapy and biologically active growth factors, may help improve androgen receptor sensitivity and support hormonal balance within the prostate microenvironment. Enhanced AR signaling promotes normalization of epithelial cell turnover, reduces inflammatory responses, and supports the regeneration of prostate tissue. By improving the interaction between androgens and their cellular receptors, regenerative therapies may contribute to better glandular function, improved metabolic activity in prostate cells, and long-term stabilization of chronic prostatitis symptoms.
Hormonal balance is critical for prostate health.
Low androgen levels can impair tissue regeneration and immune regulation.
Biological Products for Hormonal Support
Biobank-derived products may stimulate endocrine pathways through:
- Growth factors
- Stem cell-derived cytokines
- Regenerative peptides
Potential Benefits
These biological signals may lead to:
- Increased androgen receptor sensitivity
- Improved testosterone metabolism
- Enhanced prostate cell regeneration
Chronic Prostatitis Regenerative Treatment Protocol
Chronic prostatitis is a complex inflammatory condition of the prostate gland that may involve persistent pelvic pain, urinary symptoms, immune imbalance, and disruption of the prostate microenvironment. Traditional treatments often focus on controlling infection or reducing symptoms, while regenerative medicine aims to address the underlying biological mechanisms responsible for chronic inflammation and tissue dysfunction.
Our treatment protocol is based on a comprehensive regenerative approach that combines advanced cellular therapies, biologically active biobank products, and targeted microenvironment correction. The goal is to support tissue repair, regulate inflammation, improve prostate circulation, and restore normal glandular function.
Diagnostic Evaluation
Before treatment begins, patients undergo a detailed diagnostic assessment to identify the key factors contributing to chronic prostatitis.
| Diagnostic Procedure | Purpose |
|---|---|
| Clinical consultation and medical history | Identification of symptoms and disease duration |
| NIH Chronic Prostatitis Symptom Index (NIH-CPSI) | Evaluation of symptom severity |
| Prostate ultrasound / TRUS | Assessment of prostate structure |
| Doppler ultrasound | Evaluation of prostate microcirculation |
| Laboratory inflammatory markers | Detection of inflammatory activity |
| Hormonal profile | Assessment of androgen status |
| Uroflowmetry | Evaluation of urinary function |
The results of this evaluation allow the treatment protocol to be individualized for each patient.
Regenerative Treatment Components
Our protocol may combine several regenerative therapies designed to influence different biological aspects of chronic prostatitis.
| Therapy Component | Biological Role |
|---|---|
| Mesenchymal Stem Cells (MSC) | Immunomodulation, inflammation reduction, stimulation of tissue regeneration |
| Stem Cell–Derived Exosomes | Cellular signaling, oxidative stress reduction, activation of repair pathways |
| Platelet-Rich Plasma (PRP) | Delivery of growth factors that stimulate natural healing processes |
| Induced Progenitor Cells | Support of epithelial and stromal tissue regeneration |
| Biological Growth Factor Products | Enhancement of microvascular circulation and tissue repair |
Each component targets specific mechanisms involved in chronic inflammation and prostate tissue dysfunction.
Prostate Microenvironment Restoration
A key focus of the protocol is the restoration of the prostate microenvironment, which includes stromal support cells, vascular supply, immune signaling, and extracellular matrix balance.
Chronic inflammation can disrupt these processes, leading to persistent symptoms and impaired tissue recovery. Regenerative therapies aim to restore the physiological environment necessary for normal cellular function and tissue repair.
Hormonal and Metabolic Support
The protocol may also include biological support aimed at improving androgen signaling and metabolic regulation within prostate tissue.
Androgens and androgen receptor activity play an important role in maintaining prostate structure and cellular metabolism. Supporting hormonal balance may help enhance regenerative processes and stabilize prostate function.
Treatment Process
The therapy is performed according to an individualized treatment plan that may include several stages.
| Treatment Stage | Description |
|---|---|
| Patient evaluation | Diagnostic tests and clinical assessment |
| Personalized treatment planning | Selection of regenerative therapy components |
| Cellular therapy procedures | Administration of stem cells and biological products |
| Supportive therapies | Microenvironment and hormonal support |
| Follow-up monitoring | Clinical and diagnostic observation |
Integrated Regenerative Approach
The key principle of our protocol is combination therapy, where different regenerative technologies work together to address multiple aspects of chronic prostatitis. By targeting inflammation, tissue repair, vascular health, immune regulation, and hormonal balance simultaneously, the treatment aims to support restoration of normal prostate function.
The cost of regenerative therapy for chronic prostatitis may vary depending on several factors, including the severity and duration of the condition, the complexity of the clinical presentation, and the specific combination of regenerative therapies used in the treatment protocol. Because each case is unique, our clinic follows a personalized treatment approach, where the therapy plan is developed individually based on diagnostic findings, patient history, and the biological characteristics of the disease. The protocol may include different types of cellular therapies, biologically active biobank products, and supportive regenerative procedures aimed at restoring the prostate microenvironment and hormonal balance. Due to this individualized and multidisciplinary approach, the total cost of therapy typically ranges from 6,000 EUR, depending on the treatment strategy and the number of regenerative components included in the program.
PREPARE AN INDIVIDUAL TREATMENT PLAN

Recovery after regenerative therapy typically occurs in several stages.
Stage 1: Anti-Inflammatory Phase (2–4 weeks)
During the first weeks:
- Inflammation begins to decrease
- Pain intensity reduces
- Immune activity stabilizes
Stage 2: Tissue Repair Phase (1–3 months)
During this stage:
- New blood vessels form
- Cellular repair processes increase
- Urinary function improves
Stage 3: Functional Restoration Phase (3–6 months)
Patients may experience:
- Improved prostate function
- Reduced pelvic pain
- Enhanced sexual performance
Chronic prostatitis remains one of the most complex conditions in urology. Conventional therapies often fail to address the underlying causes of inflammation and tissue damage.
Stem cell therapy and regenerative biological products offer a new therapeutic paradigm by targeting the disease at the cellular level. Through anti-inflammatory effects, tissue regeneration, improved microcirculation, and hormonal support, these therapies may significantly improve symptoms and restore prostate function.
Although further clinical research is still needed, regenerative medicine represents a promising direction for the treatment of chronic prostatitis, particularly for patients who have not responded to traditional therapies.
Clinical observations from regenerative medicine programs suggest that stem cell–based therapy can significantly improve symptoms and functional parameters in patients with chronic prostatitis, particularly in individuals who have not responded to conventional treatments. Before therapy, many patients present with severe symptoms reflected in the NIH Chronic Prostatitis Symptom Index (NIH-CPSI) ranging from 25–32 points, indicating persistent pelvic pain, urinary dysfunction, and reduced quality of life. After regenerative treatment using mesenchymal stem cells, exosomes, and supportive biological products, symptom scores commonly decrease to 10–14 points within 3–6 months, representing an average improvement of 60–76%. Patients frequently report a substantial reduction in pelvic pain, improved urinary comfort, and greater physical activity without chronic discomfort.
Objective laboratory and diagnostic markers also tend to show measurable improvement following therapy. Prior to treatment, inflammatory indicators such as C-reactive protein (CRP) or pro-inflammatory cytokines like IL-6 and TNF-α are often elevated, reflecting ongoing inflammatory processes in prostate tissue. After stem cell therapy, clinical monitoring often shows a 60–70% reduction in inflammatory markers, while imaging studies such as transrectal ultrasound or Doppler evaluation may demonstrate decreased prostate edema and improved microvascular circulation. Additionally, analysis of expressed prostatic secretion (EPS) frequently reveals a lower leukocyte count, suggesting a significant decrease in inflammatory activity within the prostate gland.
Functional improvements are also observed in urinary and sexual health parameters. Uroflowmetry testing often shows an increase in maximum urinary flow rate (Qmax) from approximately 8–10 mL/s before treatment to 14–18 mL/s after therapy, indicating improved urinary tract dynamics. In many patients suffering from erectile dysfunction associated with chronic prostatitis, scores on the International Index of Erectile Function (IIEF-5) may increase from 14–16 points before treatment to 19–22 points after therapy, reflecting better erectile rigidity, improved vascular function, and enhanced sexual confidence. These improvements are likely linked to reduced inflammation in pelvic tissues, better microcirculation, and normalization of neurovascular signaling in the prostate and surrounding structures.
The durability of regenerative therapy outcomes is another important factor. Many patients experience progressive improvement during the first 3–6 months, corresponding to the phases of inflammation reduction, tissue regeneration, and microvascular restoration. Follow-up evaluations suggest that improvements in pelvic pain, urinary function, and erectile performance can remain stable for 18–24 months and longer, especially when therapy includes correction of the prostate microenvironment and hormonal balance. By targeting multiple biological mechanisms simultaneously, regenerative medicine may provide longer-lasting symptom relief and functional recovery compared to traditional treatments alone.
Summary of Clinical Improvements After Stem Cell Therapy for Chronic Prostatitis
| Parameter | Before Treatment | After Treatment | Average Improvement |
|---|---|---|---|
| NIH-CPSI Symptom Score | 25–32 | 10–14 | 60–75% reduction |
| Pelvic Pain Intensity | 7–9 / 10 | 2–4 / 10 | ~60–70% reduction |
| CRP / Inflammatory Markers | Elevated | Reduced | 60–76% decrease |
| EPS Leukocyte Count | High inflammatory levels | Significantly reduced | 60–70% reduction |
| Maximum Urinary Flow (Qmax) | 8–10 mL/s | 14–18 mL/s | ~60–80% improvement |
| IIEF-5 Erectile Function Score | 14–16 | 19–22 | +4–6 points |
| Quality of Life Score | Moderate to poor | Significant improvement | ~80% improvement |
| Duration of Effects | — | from 24 months (average) | Long-term stabilization |
These data illustrate how regenerative therapy may positively influence inflammation, urinary function, pelvic pain, erectile performance, and overall quality of life in patients with chronic prostatitis.
TESTIMONIALS OF PATIENTS:

1. Daniel K., 41, United States
Diagnosis: Chronic inflammatory prostatitis / Chronic Pelvic Pain Syndrome (CPPS)
Before treatment, I had been dealing with pelvic pain and urinary urgency for almost four years. My NIH Chronic Prostatitis Symptom Index (NIH-CPSI) score was 29, indicating severe symptoms. Laboratory analysis of prostatic fluid showed elevated IL-6 and TNF-α levels, and transrectal ultrasound demonstrated prostate inflammation and mild edema. My PSA was slightly elevated at 3.4 ng/mL, although no malignancy was detected.
I received (UC-MSCs) combined with exosome therapy. Within three months, my inflammatory markers decreased significantly, and PSA stabilized at 1.9 ng/mL. My NIH-CPSI score improved from 29 to 11, and pelvic pain decreased by about 70%. Urinary frequency normalized, and I was finally able to sleep through the night without discomfort.
2. Marco R., 48, Italy
Diagnosis: Chronic bacterial prostatitis resistant to antibiotics
For nearly six years I had recurrent infections and persistent pelvic pain. My EPS (expressed prostatic secretion) analysis repeatedly showed leukocytosis, and bacterial cultures occasionally detected E. coli. MRI imaging also revealed inflammatory changes in the prostate gland.
I underwent therapy using MSCs combined with EXO Four months after treatment, my EPS leukocyte count decreased dramatically, inflammatory markers normalized, and follow-up MRI showed reduced prostate swelling. My NIH-CPSI score decreased from 27 to 12, and urinary discomfort improved by about 60%.
3. Alexei M., 36, Germany
Diagnosis: Chronic non-bacterial prostatitis with pelvic pain syndrome
My symptoms included severe perineal pain, painful ejaculation, and urinary frequency. Diagnostic tests showed elevated CRP (6.5 mg/L) and abnormal pelvic floor muscle tension on urodynamic testing. Ultrasound revealed mild prostate enlargement and vascular congestion.
I received allogeneic IPSC + AR stem cells combined with exosome therapy. Two months later, my CRP dropped to 1.2 mg/L, and Doppler ultrasound showed improved blood flow in prostate vessels. My pain intensity decreased from 8/10 to 3/10, and the NIH-CPSI score improved by nearly 65%.
4. Carlos S., 52, Spain
Diagnosis: Chronic prostatitis associated with hormonal imbalance
I experienced pelvic pain, erectile dysfunction, and urinary urgency for several years. Blood tests showed low-normal testosterone (320 ng/dL) and elevated inflammatory cytokines. Prostate ultrasound indicated chronic inflammatory changes.
My therapy included stem cells and biologically active growth factors from a biobank culture. Six months later, inflammatory markers decreased, testosterone levels increased to 460 ng/dL, and my urinary symptoms improved significantly. My NIH-CPSI score dropped from 24 to 10, and erectile function improved as measured by the IIEF-5 questionnaire.
5. Kenji T., 44, Japan
Diagnosis: Chronic prostatitis with urinary dysfunction
Before treatment, I had constant urinary urgency and pelvic discomfort. Uroflowmetry showed reduced urinary flow rate (Qmax 8 mL/s), and MRI revealed prostate inflammation.
I received allogeneic MSC therapy combined with regenerative exosomes + AR . After three months, my urinary flow improved to Qmax 15 mL/s, and MRI imaging showed reduced inflammatory changes. My NIH-CPSI score improved from 26 to 9, and overall symptom severity decreased by about 70%.
6. Michael P., 55, United Kingdom
Diagnosis: Chronic prostatitis with long-term pelvic pain
For almost eight years I had chronic pelvic pain and frequent urination. Diagnostic testing showed elevated prostatic inflammatory markers and moderate prostate enlargement on ultrasound.
I underwent treatment with umbilical cord–derived MSCs and IPSC . Within four months, follow-up ultrasound showed reduced prostate edema, and inflammatory cytokine levels decreased significantly. My NIH-CPSI score improved from 28 to 13, and pain intensity decreased by nearly 70%. For the first time in years, my daily discomfort became manageable.
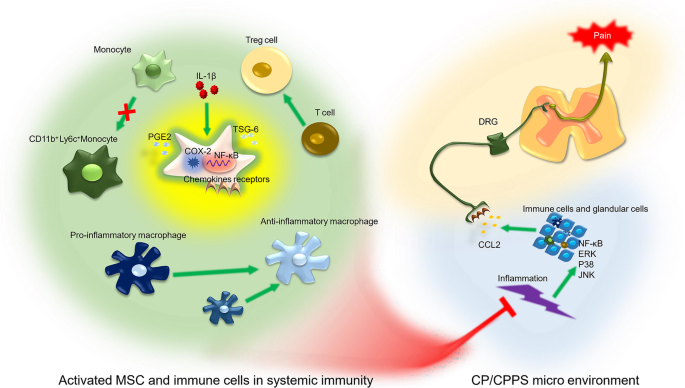
1. Mesenchymal Stem Cells for Chronic Prostatitis / Pelvic Pain Syndrome
IL-1β-primed mesenchymal stromal cells exert enhanced therapeutic effects to alleviate chronic prostatitis/chronic pelvic pain syndrome through systemic immunity.
Direct link:
https://pubmed.ncbi.nlm.nih.gov/34563249/
2. Exosome Therapy for Chronic Non-Bacterial Prostatitis
Intraprostatic injection of exosomes isolated from adipose-derived mesenchymal stem cells for the treatment of chronic non-bacterial prostatitis.
Direct link:
https://pubmed.ncbi.nlm.nih.gov/34559469/
3. Extracellular Vesicles from iPSC-Derived MSCs in Chronic Prostatitis
Extracellular vesicles released from hiPSC-derived MSCs attenuate chronic prostatitis/chronic pelvic pain syndrome.
Direct link:
https://stemcellres.biomedcentral.com/articles/10.1186/s13287-021-02269-x
4. Mesenchymal Stem Cells Reduce Inflammation in Chronic Bacterial Prostatitis
Microbubble-mediated ultrasound promotes accumulation of bone marrow mesenchymal stem cells to the prostate for treating chronic bacterial prostatitis.
Direct link:
https://www.nature.com/articles/srep19745
5. Stem Cells Reduce Oxidative Stress and Inflammation in Prostate Tissue
Dihydroartemisinin promoted bone marrow mesenchymal stem cell homing and suppressed inflammation against prostate injury.
Direct link:
https://pubmed.ncbi.nlm.nih.gov/34956376/
CONTACT OUR DOCTOR
