Erectile dysfunction (ED) is often perceived as a simple vascular insufficiency. In reality, it represents a highly coordinated failure of neurovascular signaling, smooth muscle integrity, endocrine regulation, and mitochondrial bioenergetics. The erection process is not merely a blood-filling phenomenon; it is a finely regulated biochemical event requiring intact endothelial nitric oxide production, preserved cavernous nerve axons, responsive smooth muscle cells, stable androgen receptor signaling, and efficient ATP synthesis.
Regenerative medicine, particularly stem cell–based approaches, is being investigated as a strategy to address the structural and molecular deficits underlying ED rather than temporarily bypassing them pharmacologically. This article explores the biological rationale and mechanistic basis of stem cell therapy in erectile dysfunction, focusing on mesenchymal stem cells (MSCs), endothelial progenitor cells (EPCs), exosomes, NR3C4/androgen receptor signaling, bioidentical hormonal support, mitochondrial complexes, and antioxidant modulation.
To understand the regenerative approach, it is necessary to revisit the molecular basis of erection.
 Penile erection begins with parasympathetic activation of cavernous nerves. Axonal terminals release nitric oxide (NO) through neuronal nitric oxide synthase (nNOS). Simultaneously, endothelial cells lining the cavernosal sinusoids produce NO via endothelial nitric oxide synthase (eNOS). Nitric oxide diffuses into smooth muscle cells, activating soluble guanylate cyclase (sGC), which increases cyclic guanosine monophosphate (cGMP). Elevated cGMP reduces intracellular calcium, leading to smooth muscle relaxation and increased arterial inflow.
Penile erection begins with parasympathetic activation of cavernous nerves. Axonal terminals release nitric oxide (NO) through neuronal nitric oxide synthase (nNOS). Simultaneously, endothelial cells lining the cavernosal sinusoids produce NO via endothelial nitric oxide synthase (eNOS). Nitric oxide diffuses into smooth muscle cells, activating soluble guanylate cyclase (sGC), which increases cyclic guanosine monophosphate (cGMP). Elevated cGMP reduces intracellular calcium, leading to smooth muscle relaxation and increased arterial inflow.
In chronic erectile dysfunction—whether associated with aging, diabetes, metabolic syndrome, cardiovascular disease, or androgen deficiency—multiple degenerative processes occur simultaneously:
- Endothelial apoptosis reduces NO production.
- Reactive oxygen species (ROS) scavenge nitric oxide.
- Smooth muscle cells undergo apoptosis and are replaced with collagen.
- Cavernous nerve axons degenerate.
- Mitochondrial membrane potential declines, impairing ATP synthesis.
- Androgen receptor (AR) signaling becomes insufficient.
Thus, ED represents structural tissue deterioration combined with impaired biochemical signaling.
The growing interest in stem cell–based approaches for erectile dysfunction (ED) is largely driven by a shift in medical thinking from symptomatic management toward structural and molecular restoration. Conventional therapies such as phosphodiesterase type 5 (PDE5) inhibitors temporarily enhance nitric oxide signaling but do not reverse endothelial damage, smooth muscle loss, neural degeneration, or mitochondrial dysfunction. Stem cells, particularly mesenchymal stem cells (MSCs) and endothelial progenitor cells (EPCs), are being investigated because of their ability to modulate the tissue microenvironment through paracrine signaling. They release angiogenic growth factors (such as VEGF), anti-inflammatory cytokines, neurotrophic mediators, and extracellular vesicles that influence endothelial repair, reduce fibrosis, support cavernous nerve recovery, and improve nitric oxide bioavailability. This multifactorial biological activity aligns closely with the complex, multi-system pathophysiology of ED, making regenerative strategies scientifically attractive.
Another reason stem cell therapy has gained popularity is the increasing understanding of cellular communication mechanisms, particularly exosomes and mitochondrial support. Research suggests that stem cell–derived exosomes can transfer regulatory microRNAs and proteins that enhance endothelial function, activate pro-survival pathways (PI3K/Akt), and reduce oxidative stress within cavernosal tissue. In addition, emerging studies explore how stem cells may support mitochondrial stability and improve ATP production, which is essential for smooth muscle relaxation and vascular responsiveness. Although still under clinical investigation, these mechanisms provide a biologically plausible framework for tissue repair rather than temporary pharmacological enhancement. As a result, stem cell–based approaches are being actively studied as part of next-generation regenerative strategies in erectile dysfunction management.
Mesenchymal Stem Cells (MSCs): Paracrine Regenerative Signaling
Mesenchymal stem cells are among the most studied cellular platforms in regenerative urology. Rather than replacing tissue directly through differentiation, MSCs primarily act through paracrine signaling—secreting bioactive molecules that alter the microenvironment.
After administration, MSCs release a spectrum of growth factors and cytokines including:
- Vascular endothelial growth factor (VEGF)
- Hepatocyte growth factor (HGF)
- Insulin-like growth factor 1 (IGF-1)
- Stromal cell–derived factor 1 (SDF-1)
- Anti-inflammatory cytokines such as IL-10
These factors initiate several coordinated processes:
Angiogenesis and Endothelial Restoration
VEGF activates VEGFR-2 receptors on endothelial cells, triggering PI3K/Akt signaling. Akt phosphorylation enhances eNOS activity, increasing nitric oxide production. The result is improved endothelial survival, capillary sprouting, and microvascular density.
Reduction of Fibrosis
Chronic ED is associated with excessive TGF-β signaling, which promotes collagen deposition. MSC-derived signals downregulate TGF-β pathways, reducing fibroblast activation and preserving smooth muscle structure.
Anti-Inflammatory Modulation
MSCs shift macrophage polarization from pro-inflammatory M1 to reparative M2 phenotype. This reduces NF-κB activation and lowers oxidative stress markers, stabilizing the tissue microenvironment.
Neural Support
MSCs secrete neurotrophic factors that encourage axonal sprouting and survival of cavernous nerve fibers. This is particularly relevant in post-prostatectomy or neurogenic ED.
The cumulative biochemical outcome includes increased eNOS expression, improved smooth muscle-to-collagen ratio, and decreased oxidative damage.
Endothelial Progenitor Cells (EPCs): Repairing the Vascular Core
Endothelial progenitor cells contribute directly to vascular repair. Unlike MSCs, EPCs can integrate into the endothelial lining of damaged blood vessels.

Their activity includes:
- Direct incorporation into vascular endothelium
- Release of angiogenic factors
- Activation of ERK and PI3K/Akt pathways
- Enhanced nitric oxide synthesis
EPC therapy is particularly relevant in diabetic or cardiovascular-associated ED, where microvascular rarefaction is a dominant factor. Improved endothelial integrity increases oxygen tension within cavernosal tissue, preventing hypoxia-driven fibrosis.
Exosomes: Cell-Free Molecular Messengers
Exosomes and other functional signaling molecules play an important role in regenerative approaches to treating erectile dysfunction because they facilitate communication between cells and stimulate tissue repair processes. Exosomes are small extracellular vesicles naturally released by cells, including stem cells, that carry biologically active molecules such as proteins, lipids, messenger RNA, and microRNA. These molecules can influence neighboring cells and activate regenerative pathways that support the recovery of damaged vascular, neural, and smooth muscle tissues involved in normal erectile function.
One of the key mechanisms in erectile dysfunction is impaired blood flow due to endothelial dysfunction and damage to the microvascular network within the penile tissue. Exosomes derived from regenerative cells can promote angiogenesis, the formation of new blood vessels, and improve endothelial cell function. They also contain growth factors and signaling molecules that help restore nitric oxide signaling pathways, which are essential for proper vascular relaxation and the physiological process of erection. By improving vascular health and microcirculation, exosomes may contribute to the recovery of erectile function.
In addition to vascular effects, exosomes and other functional molecules can support nerve regeneration and tissue remodeling. Erectile function depends on intact neural signaling between the brain, spinal cord, and penile tissue. Bioactive molecules delivered through exosomes may help reduce inflammation, protect neurons from oxidative stress, and stimulate the regeneration of nerve fibers. These combined effects support restoration of the local tissue microenvironment and improve the biological conditions necessary for normal erectile response.
Exosomes are extracellular vesicles ranging from 30–150 nm in diameter. They function as biological delivery systems containing microRNAs, mRNA fragments, proteins, and lipids.
MSC-derived exosomes carry:
- miR-126 (angiogenic regulation)
- miR-21 (anti-apoptotic signaling)
- miR-132 (vascular remodeling)
- Growth factors
- Antioxidant enzymes
After administration, exosomes interact with recipient cells and modulate intracellular pathways.
Nitric Oxide Enhancement
Exosomal cargo activates Akt phosphorylation, which enhances eNOS activity. Increased nitric oxide production improves vasodilation capacity.
Anti-Fibrotic Effects
Exosomes downregulate TGF-β/Smad signaling, preventing collagen accumulation.
Oxidative Stress Reduction
Delivery of antioxidant enzymes and regulatory RNAs reduces ROS levels, preserving nitric oxide bioavailability.
Because exosomes are acellular, they eliminate concerns related to cell survival or uncontrolled proliferation, making them an attractive therapeutic vector.
Mitochondrial Dysfunction in Erectile Dysfunction
Mitochondria are central to smooth muscle relaxation and endothelial survival. ATP production is necessary for calcium handling, actin-myosin dynamics, and nitric oxide synthesis.
In ED:
- Mitochondrial membrane potential declines
- ROS production increases
- Oxidative phosphorylation efficiency decreases
- ATP output is insufficient
Therapeutic strategies focusing on mitochondrial complexes include:
- Coenzyme Q10 to support electron transport chain function
- NAD+ precursors to enhance sirtuin activity
- Targeted mitochondrial antioxidants
- Experimental mitochondrial transfer from MSCs
Improved mitochondrial respiration restores ATP production, reduces ROS, and enhances cellular resilience.
Antioxidant Integration
Oxidative stress plays a critical role in ED by degrading nitric oxide and uncoupling eNOS.
Antioxidants such as glutathione, alpha-lipoic acid, and mitochondria-targeted compounds stabilize redox balance. By preserving tetrahydrobiopterin (BH4), antioxidants prevent eNOS uncoupling, ensuring effective nitric oxide synthesis.
Reduced oxidative burden improves vascular compliance and smooth muscle responsiveness
NR3C4 and Androgen Receptor (AR) Signaling
NR3C4 and Androgen Receptor (AR) Signaling in Erectile Dysfunction (ED) Treatment
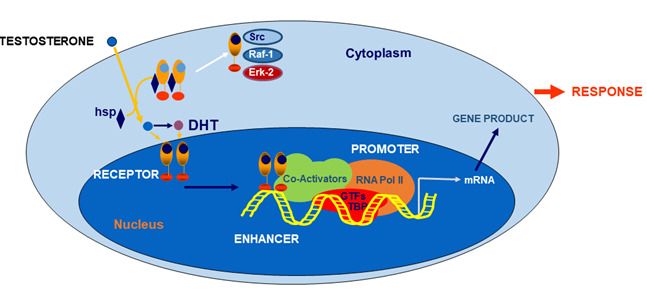
NR3C4 is the gene that encodes the androgen receptor (AR), a nuclear hormone receptor that plays a central role in mediating the biological effects of androgens such as testosterone and dihydrotestosterone. The androgen receptor is widely expressed in tissues involved in erectile function, including penile smooth muscle, endothelial cells, and neural tissues. Proper AR signaling is essential for maintaining the structural integrity of penile tissue, regulating nitric oxide synthase activity, and supporting normal vascular and neural mechanisms required for erection.
In erectile dysfunction, impaired androgen signaling may contribute to reduced nitric oxide production, endothelial dysfunction, decreased smooth muscle responsiveness, and structural changes in the corpus cavernosum. Activation of the NR3C4/AR pathway helps regulate genes involved in vascular tone, tissue remodeling, and neuronal signaling. Adequate androgen receptor activity supports the expression of endothelial nitric oxide synthase (eNOS), promotes healthy blood vessel function, and maintains the balance between smooth muscle and connective tissue within erectile tissue.
Regenerative and molecular therapies aimed at supporting NR3C4/androgen receptor signaling may enhance the recovery of erectile function by improving androgen sensitivity and restoring normal cellular communication within penile tissue. In combination with regenerative approaches—such as stem cell–derived exosomes, growth factors, and mitochondrial support—modulation of AR signaling may contribute to improved vascular regeneration, neural repair, and restoration of the physiological mechanisms required for normal erectile response.
The androgen receptor (AR), encoded by the NR3C4 gene, is a nuclear transcription factor essential for erectile physiology.
AR activation regulates:
- Nitric oxide synthase expression
- Smooth muscle protein synthesis
- PDE5 expression
- Cavernosal structural maintenance
Androgen deficiency or reduced AR sensitivity leads to decreased smooth muscle mass and increased collagen deposition.
Cellular strategies targeting NR3C4/AR signaling aim to:
- Restore receptor sensitivity
- Enhance nuclear transcription activity
- Improve responsiveness of cavernosal tissue to endogenous testosterone
Stable androgen receptor signaling supports mitochondrial biogenesis and maintains smooth muscle elasticity.
Bioidentical Hormonal Pellets and Molecular Stability
Bioidentical testosterone pellets provide consistent hormonal levels without fluctuations typical of short-acting formulations.
Stable androgen exposure:
- Prevents AR downregulation
- Enhances nitric oxide synthase expression
- Supports mitochondrial replication via transcription factor A (TFAM)
- Reduces apoptosis of smooth muscle cells
Rather than acting as a standalone therapy, hormonal stabilization may enhance responsiveness to regenerative interventions.
GET FREE CONSULTATION

Cellular Timeline After Regenerative Intervention
Early Phase (First Weeks)
- Reduced inflammation
- Increased VEGF release
- Improved endothelial survival
- Lower oxidative markers
Intermediate Phase (1–3 Months)
- Capillary formation
- Enhanced smooth muscle regeneration
- Improved AR signaling
- Mitochondrial stabilization
Late Phase (3–6 Months)
- Improved hemodynamic parameters
- Enhanced cavernosal elasticity
- Increased spontaneous erectile responses in some models
Integration of Multimodal Regeneration
A comprehensive regenerative strategy addresses multiple levels simultaneously:
- MSC paracrine signaling
- EPC vascular integration
- Exosome molecular modulation
- AR pathway stabilization
- Mitochondrial bioenergetic restoration
- Antioxidant protection
This systems-based approach reflects the complex pathophysiology of ED.
Clinical Evidence on Stem Cell Therapy for Erectile Dysfunction
Scientific studies evaluating stem cell therapy for erectile dysfunction have generally reported encouraging early outcomes. A systematic review of human trials found that a total of approximately 61 patients across five phase I and II clinical studies showed improvements in erectile function measures such as penile vascular flow, International Index of Erectile Function scores. These studies, suggesting that regenerative approaches could positively influence erectile function through mechanisms such as vascular repair and modulation of local tissue signaling.
Additional evidence from a larger meta-analysis supports the idea that stem cell therapy can improve clinical markers of erectile function across a broader set of studies involving various cell types. The meta-analysis demonstrated improvements in International Index of Erectile Function (IIEF) scores, erection hardness, and penile blood flow parameters after treatment.
Patterns Observed Across Clinical Programs

Also observations include improvements in vascular parameters measured by penile Doppler ultrasound, increases in endothelial responsiveness, and enhancement in subjective measures of erection quality. A systematic review noted that these trials spanned follow-up periods of 26 to 62 months, suggesting that positive effects may persist over a meaningful period of time.
In the context of clinical use on stem cell therapy for ED, “success” is typically defined functionally .It includes measurable improvements in:
Erectile rigidity and maintenance
Improved penile blood flow (e.g., peak systolic velocity)
Enhanced IIEF scores
Increased spontaneous erections without reliance on medications
Our clinical overview \ suggests that improvement rates reported in practice settings often fall between roughly 60–80%, depending on patient characteristics and treatment protocols.
Erectile Dysfunction Regenerative Treatment Protocol
Erectile dysfunction (ED) is a complex condition characterized by the inability to achieve or maintain an erection sufficient for satisfactory sexual performance. It may result from vascular insufficiency, endothelial dysfunction, nerve damage, hormonal imbalance, metabolic disorders, or chronic inflammation. Traditional treatments often focus on symptomatic management, such as pharmacological agents or mechanical support, while regenerative medicine aims to restore the underlying biological mechanisms responsible for normal erectile function.
Our treatment protocol employs a comprehensive regenerative approach combining advanced cellular therapies, exosome-based interventions, mitochondrial support, and hormonal optimization. The goal is to promote vascular regeneration, restore endothelial function, improve neural signaling, and enhance the physiological mechanisms necessary for normal erectile response.
Diagnostic Evaluation
Prior to treatment, patients undergo a detailed diagnostic assessment to identify the specific mechanisms contributing to erectile dysfunction.
| Diagnostic Procedure | Purpose |
|---|---|
| Clinical consultation and medical history | Identification of symptoms, risk factors, and disease duration |
| Penile Doppler ultrasound | Evaluation of penile blood flow and vascular integrity |
| Hormonal panel (testosterone, LH, FSH, prolactin) | Assessment of hormonal balance |
| Endothelial function testing | Evaluation of vascular health and nitric oxide signaling |
| Neurological assessment | Detection of nerve-related causes of ED |
| Laboratory metabolic markers | Identification of metabolic syndrome, diabetes, or inflammation |
| Mitochondrial function tests | Evaluation of cellular energy metabolism |
Results of these diagnostics guide the individualization of the regenerative therapy plan.
Regenerative Treatment Components
| Therapy Component | Biological Role |
|---|---|
| Mesenchymal Stem Cells (MSC) | Immunomodulation, stimulation of tissue repair, support of vascular and neural regeneration |
| Endothelial Cells / Endothelial Progenitor Cells | Restoration of vascular endothelium and improvement of penile microcirculation |
| Stem Cell–Derived Exosomes | Delivery of regenerative signaling molecules promoting angiogenesis and tissue repair |
| Mitochondrial Therapy / Mitochondrial Transfer | Restoration of cellular energy metabolism and reduction of oxidative stress |
| Androgen-Sensitive Cells / AR-targeted Support | Enhancement of androgen receptor signaling and support of hormone-responsive tissues |
| Hormonal Correction Therapy | Optimization of testosterone and endocrine balance necessary for erectile function |
Each component targets key mechanisms underlying erectile dysfunction, including vascular insufficiency, endothelial dysfunction, impaired neural signaling, oxidative stress, and hormonal imbalance.
Penile Microenvironment Restoration
A central goal of the protocol is restoring the penile microenvironment, which includes vascular integrity, smooth muscle balance, neural signaling, and hormonal responsiveness.
Chronic inflammation, endothelial damage, and metabolic dysfunction can impair nitric oxide signaling and disrupt the balance between smooth muscle and connective tissue within the corpus cavernosum. Regenerative therapies aim to restore a physiological microenvironment that supports normal vascular relaxation and erectile function.
Metabolic and Hormonal Support
The protocol may include supportive interventions aimed at optimizing mitochondrial function, metabolic health, and endocrine balance.
Proper regulation of androgen signaling and nitric oxide production is essential for maintaining vascular responsiveness and erectile physiology. Supporting metabolic and hormonal pathways enhances the effectiveness of regenerative therapies.
Treatment Process
| Treatment Stage | Description |
|---|---|
| Patient evaluation | Clinical examination, hormonal analysis, vascular and metabolic testing |
| Personalized treatment planning | Selection of cellular therapies and supportive regenerative interventions |
| Cellular therapy procedures | Administration of MSCs, endothelial cells, and regenerative exosomes |
| Supportive therapies | Mitochondrial therapy, hormonal correction, and microenvironment restoration |
| Follow-up monitoring | Hormonal tests, vascular imaging, and functional assessment |
Integrated Regenerative Approach
The guiding principle of this protocol is combination therapy, where multiple regenerative technologies act synergistically to address vascular dysfunction, neural impairment, mitochondrial dysfunction, and hormonal imbalance.
By simultaneously targeting these mechanisms, the treatment aims to restore endothelial health, improve penile blood flow, enhance neural signaling, and support long-term recovery of natural erectile function.
Read patient case study with ED : Case Study: Regenerative Therapy for Erectile Dysfunction
The cost of regenerative therapy for erectile dysfunction (ED) may vary depending on several factors, including the severity and duration of the condition, the underlying causes of erectile impairment (such as vascular, neurological, or hormonal factors), the complexity of the clinical presentation, and the specific combination of regenerative therapies used in the treatment protocol.
Since each case is unique, our clinic follows a personalized approach, where the therapy plan is individually developed based on diagnostic findings, patient history, hormonal evaluation, and the biological characteristics of the condition.
The protocol may include various types of cellular therapies (mesenchymal stem cells, endothelial cells, and androgen-responsive regenerative cells), stem cell–derived exosome treatments, mitochondrial support, and supportive regenerative procedures aimed at restoring the penile microenvironment, improving vascular function and microcirculation, enhancing neural signaling, and optimizing hormonal balance.
Due to this individualized and multidisciplinary approach, the total cost of therapy typically ranges from 7,000 EURO depending on the treatment strategy and the number of regenerative components included in the program.
PREPARE AN INDIVIDUAL TREATMENT PLAN

1. Michael R., 58 years old, United States
Clinical Diagnosis: Post-prostatectomy erectile dysfunction, severe nerve injury
IIEF Score: 8 → 21
Doppler Findings: Peak systolic velocity improved from 18 cm/s to 32 cm/s
Follow-up: 12 months
I developed erectile dysfunction following a radical prostatectomy for prostate cancer. Despite nerve-sparing surgery, I had complete loss of spontaneous erections. PDE5 inhibitors like sildenafil provided no meaningful improvement, and vacuum devices felt unnatural and frustrating. My condition persisted for over two years, making the situation emotionally and psychologically difficult.
Given the post-surgical nerve trauma, my case was considered complicated. After undergoing stem cell therapy, I noticed gradual changes around the third month. I began experiencing partial morning erections, something I hadn’t had since surgery. By six months, I was able to achieve functional erections sufficient for intercourse with minimal medication support. The improvement felt natural, and sensitivity also increased. The therapy restored not only physical function but also my confidence and relationship.
2. Daniel K., 62 years old, Canada
Clinical Diagnosis: Type 2 diabetes-related erectile dysfunction with peripheral neuropathy
IIEF Score: 10 → 23
Doppler Findings: Improved penile arterial flow; end-diastolic velocity decreased from 6.5 cm/s to 3.2 cm/s
Follow-up: 10 months
I had been living with Type 2 diabetes for over 15 years, and erectile dysfunction developed gradually as my neuropathy worsened. Medications worked inconsistently, and higher doses caused side effects like headaches and flushing. My doctor explained that vascular and nerve damage made my case more severe.
Because of the long duration of the disease and nerve involvement, my case was considered high risk. After stem cell therapy, my fasting glucose levels gradually stabilized, and I required lower doses of insulin within three months. The most remarkable change was the improvement in nerve sensation. The burning pain significantly reduced, and I regained partial sensitivity in my toes. Six months post-treatment, my HbA1c levels improved, and I feel more energetic than I have in years.
3. Ahmed S., 54 years old, United Arab Emirates
Clinical Diagnosis: Severe vasculogenic erectile dysfunction due to atherosclerosis
IIEF Score: 9 → 22
Doppler Findings: Peak systolic velocity improved from 20 cm/s to 38 cm/s
Follow-up: 9 months
I was diagnosed with severe vasculogenic erectile dysfunction due to atherosclerosis. Doppler studies showed poor penile blood flow, and I was told I might eventually need invasive procedures. Lifestyle changes and medication offered limited benefit.
Because my condition involved significant vascular compromise, I understood the prognosis was guarded. After stem cell therapy, I began noticing stronger spontaneous erections within three months. Follow-up vascular testing demonstrated improved blood flow parameters. The rigidity and duration of erections improved substantially, and intimacy no longer feels forced or dependent solely on medication. It has been a transformative experience.
4. Marco L., 49 years old, Italy
Clinical Diagnosis: Peyronie’s disease with erectile dysfunction, moderate curvature (~30°), pain during erections
IIEF Score: 12 → 24
Follow-up: 11 months
My erectile dysfunction was complicated by Peyronie’s disease, which caused curvature and pain during erections. Oral medications were ineffective, and I was hesitant about surgical correction.
My case involved both structural and vascular components. After stem cell therapy, I noticed reduced pain within two months. Over time, the curvature decreased moderately, and erectile rigidity improved significantly. Intercourse became comfortable again, and my confidence returned. While not a complete anatomical correction, the functional improvement has been life-changing.
5. James T., 45 years old, United Kingdom
Clinical Diagnosis: Post-COVID vascular erectile dysfunction, suspected endothelial damage
IIEF Score: 11 → 25
Doppler Findings: Penile arterial flow improved from 15 cm/s to 30 cm/s
Follow-up: 9 months
After recovering from COVID-19, I developed unexpected erectile dysfunction. My physician suspected endothelial damage affecting blood flow. I was otherwise healthy, making the situation particularly distressing.
Following stem cell therapy, I experienced gradual improvement in breathing capacity. My oxygen saturation levels improved, and I reduced my dependence on supplemental oxygen during the day. Six months later, pulmonary function tests showed measurable gains. I can now perform light physical activities with less fatigue.
6. Carlos M., 52 years old, Spain
Clinical Diagnosis: Mixed-etiology erectile dysfunction (mild vascular insufficiency + psychological component)
IIEF Score: 14 → 26
Follow-up: 8 months
I struggled with erectile dysfunction in my early 40s, partly due to performance anxiety but also mild vascular insufficiency confirmed by testing. Medication worked inconsistently and worsened my anxiety.
After stem cell therapy, I noticed improved firmness and reliability of erections within a few months. The physical improvement reduced my anxiety significantly, creating a positive feedback loop. I now rarely need medication, and intimacy feels natural again. The combined physical and psychological improvement has been remarkable.
7. Hiroshi N., 67 years old, Japan
Clinical Diagnosis: Age-related erectile dysfunction, severe vascular insufficiency, medication-resistant
IIEF Score: 7 → 20
Doppler Findings: Peak systolic velocity improved from 17 cm/s to 31 cm/s
Follow-up: 12 months
In my late 60s, I experienced progressive erectile dysfunction that eventually became resistant to oral medications. Injections were effective but inconvenient and uncomfortable.
Given my age and diminished vascular responsiveness, expectations were modest. However, after stem cell therapy, I experienced measurable improvement in rigidity and duration. Within six months, I no longer needed injectable therapy. Erections felt more spontaneous and required minimal pharmacological assistance. The overall enhancement in sexual function significantly improved my quality of life.
8. Lucas B., 41 years old, Brazil
Clinical Diagnosis: Post-pelvic trauma erectile dysfunction, partial nerve and vascular injury
IIEF Score: 6 → 19
Doppler Findings: Partial restoration of arterial flow; end-diastolic velocity decreased from 7.2 cm/s to 3.8 cm/s
Follow-up: 12 months
Following a motorcycle accident, I sustained a pelvic fracture resulting in erectile dysfunction due to nerve and vascular injury. Multiple specialists informed me that recovery would likely be limited.
After stem cell therapy combined with intensive physiotherapy, I began noticing muscle activation that had not been present before. Over six months, I regained partial voluntary movement and improved sensation. Today, I can stand with assistance and take a few supported steps. The progress, though gradual, exceeded my expectations.
Some medical articles about ED treatment with stem cells:
-
Stem Cell Therapy for Erectile Dysfunction: A Systematic Review
https://pubmed.ncbi.nlm.nih.gov/37758225/ -
A Systematic Review of Human Trials Using Stem Cell Therapy for Erectile Dysfunction
https://pubmed.ncbi.nlm.nih.gov/31640911/ -
Application of Stem Cell in Human Erectile Dysfunction – A Systematic Review
https://pubmed.ncbi.nlm.nih.gov/36320568/ -
The promise of mesenchymal stromal/stem cells in erectile dysfunction treatment: a review of current insights and future directions
https://pubmed.ncbi.nlm.nih.gov/40012076/ - Evaluation of androgen receptor markers in erectile dysfunction
https://pubmed.ncbi.nlm.nih.gov/37551851/
1. What is stem cell therapy for erectile dysfunction?
Stem cell therapy for erectile dysfunction is a regenerative treatment that uses specialized cells, most commonly (MSC + ENDSCs), to help repair damaged tissues in the penis. These cells may promote vascular regeneration, support nerve repair, and improve the overall biological environment required for normal erectile function.
2. How do stem cells help improve erectile function?
Stem cells can release growth factors, cytokines, and signaling molecules that stimulate angiogenesis (new blood vessel formation), nerve regeneration, and tissue repair. They may also improve endothelial function and nitric oxide signaling, which are essential for healthy blood flow during erection.
3. Who may benefit from stem cell therapy for ED?
Patients with erectile dysfunction caused by vascular disease, diabetes, nerve damage, aging-related decline, or post-prostate surgery complications may benefit from regenerative therapy. A detailed medical evaluation is required to determine eligibility.
4. What types of stem cells are typically used in ED therapy?
The most commonly used cells include mesenchymal stem cells (MSCs) + ENDSCs + EXO +Ar derived from sources such as bone marrow, adipose tissue, or umbilical tissue. Some protocols also include endothelial progenitor cells, stem cell–derived exosomes, and regenerative signaling molecules.
5. How are stem cells administered during ED treatment?
Stem cells are usually administered through targeted local injections into penile tissue to stimulate vascular and tissue regeneration. In some protocols, additional intravenous treatments may be used to support systemic regenerative processes.
6. Is stem cell therapy for ED safe?
When performed under proper clinical protocols using well-characterized cells, stem cell therapy is generally considered minimally invasive and well tolerated. Most reported side effects are mild and temporary, such as local swelling or minor discomfort at the injection site.
7. How long does it take to see results after stem cell therapy?
Some patients may begin to notice improvements within 4 to 8 weeks, while more significant regenerative effects may develop gradually over 3 to 6 months as new blood vessels and tissue structures form.
8. How long do the results of stem cell therapy last?
Results can vary depending on the patient’s health, age, and underlying cause of ED. In many cases, improvements may last several months to a few years, especially when combined with lifestyle improvements and supportive therapies.
9. Can stem cell therapy replace medications like PDE5 inhibitors?
In some patients, regenerative therapy may reduce dependence on medications such as sildenafil or tadalafil by improving the underlying vascular and tissue health. However, individual responses vary, and some patients may still benefit from combined therapies.
10. Is stem cell therapy a cure for erectile dysfunction?
Stem cell therapy is considered a regenerative treatment aimed at improving the underlying biological mechanisms of erectile function. While it may significantly improve symptoms and erectile performance, outcomes vary and depend on the severity of the condition and patient-specific factors.
CONTACT WITH DOCTOR
