
Why Lichen Sclerosus Remains One of the Most Challenging Chronic Inflammatory Diseases
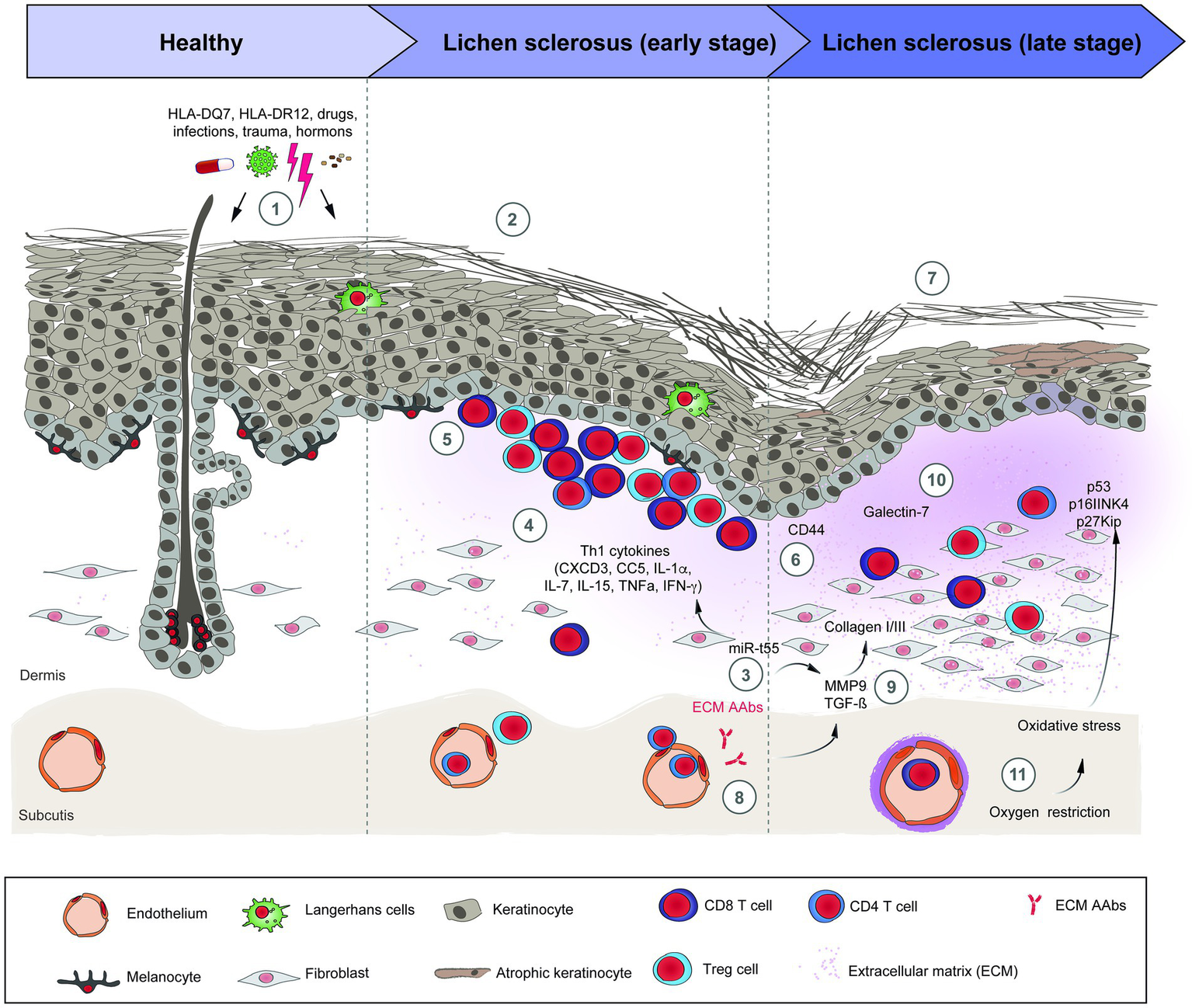
Lichen sclerosus (LS) is a chronic inflammatory dermatosis characterized by progressive sclerosis, connective tissue remodeling, epithelial atrophy, persistent immune activation, and gradual destruction of normal skin architecture. Although traditionally classified as a dermatological disorder, current research demonstrates that lichen sclerosus represents a far more complex disease involving immune dysregulation, chronic inflammation, microvascular dysfunction, extracellular matrix remodeling, and aberrant tissue repair.
Over the last two decades, significant advances in molecular biology have transformed our understanding of this condition. Instead of considering LS merely as a localized inflammatory skin disease, scientists increasingly recognize it as a disorder of tissue homeostasis in which persistent inflammation continuously disrupts the balance between tissue injury and regeneration. As inflammation progresses, normal regenerative mechanisms become exhausted, fibroblasts become chronically activated, collagen deposition accelerates, and irreversible fibrosis gradually replaces healthy functional tissue.
This concept explains one of the greatest clinical challenges encountered by physicians treating lichen sclerosus: conventional therapies are often effective in suppressing symptoms but rarely restore the biological integrity of damaged tissue. Even when inflammation temporarily subsides, the underlying pathological microenvironment frequently persists, creating favorable conditions for disease recurrence.
Consequently, regenerative medicine has emerged as one of the most promising research directions for patients with chronic inflammatory and fibrotic disorders, including lichen sclerosus. Rather than focusing exclusively on suppressing inflammation, regenerative approaches aim to restore tissue homeostasis by influencing immune regulation, angiogenesis, extracellular matrix remodeling, stem cell niches, and intercellular communication.
Among these emerging technologies, mesenchymal stem cells (MSCs), adipose-derived stem cells (ADSCs), Muse cells, extracellular vesicles, exosomes, secretome therapy, mitochondrial transfer, and immune modulation have attracted considerable scientific interest because of their ability to influence multiple biological pathways simultaneously.
Unlike traditional pharmacological agents that generally target a single inflammatory cascade, regenerative biological therapies interact with complex cellular networks, producing coordinated effects across numerous signaling pathways involved in tissue repair.
Although many of these technologies remain under active clinical investigation and are not yet established as standard treatments for lichen sclerosus, accumulating experimental and early clinical evidence suggests that they may eventually contribute to new therapeutic strategies aimed at restoring tissue function rather than simply controlling symptoms. Read full Stem cells protocol of HSV treatment : Stem Cell Treatment for Herpes Virus: Regenerative; Immune-Modulating Therapy
 Understanding Lichen Sclerosus: Beyond a Skin Disease
Understanding Lichen Sclerosus: Beyond a Skin Disease
 Understanding Lichen Sclerosus: Beyond a Skin Disease
Understanding Lichen Sclerosus: Beyond a Skin DiseaseFor many years, lichen sclerosus was regarded primarily as a chronic inflammatory skin condition of unknown origin. Today, this simplistic view has evolved considerably.
Current scientific evidence indicates that LS represents a multifactorial disorder involving interactions between:
- autoimmune dysregulation;
- genetic susceptibility;
- chronic inflammation;
- hormonal influences;
- oxidative stress;
- extracellular matrix remodeling;
- vascular dysfunction;
- impaired regenerative capacity.
These interconnected mechanisms create a self-perpetuating cycle in which inflammation continuously damages the extracellular matrix, stimulates fibroblast activation, promotes collagen accumulation, and progressively replaces healthy tissue with dense fibrotic scar tissue.
As fibrosis advances, tissue elasticity decreases, vascular perfusion deteriorates, and normal epithelial regeneration becomes increasingly impaired. Eventually, this process produces the characteristic white atrophic plaques, architectural distortion, fissuring, chronic pain, and sexual dysfunction commonly observed in advanced lichen sclerosus.
Importantly, fibrosis is not merely a cosmetic alteration. It represents profound biological remodeling affecting virtually every structural component of the affected tissue, including collagen fibers, elastic fibers, blood vessels, lymphatic vessels, peripheral nerves, immune cells, fibroblasts, stem cell niches, and epithelial progenitor cells.
This explains why advanced disease often becomes resistant to conventional anti-inflammatory medications.
Epidemiology: A Disease More Common Than Previously Believed
Lichen sclerosus affects individuals of all ages, although women are diagnosed significantly more frequently than men.
The disease demonstrates two characteristic incidence peaks:
- prepubertal girls;
- postmenopausal women.
However, increasing awareness among clinicians has revealed that LS may also occur in:
- reproductive-age women;
- adolescent boys;
- adult men;
- elderly patients.
Recent epidemiological studies suggest that the true prevalence is substantially underestimated because many patients remain undiagnosed for years.
Several factors contribute to delayed diagnosis:
Patients often attribute early itching to fungal infections, allergic dermatitis, eczema, or simple skin irritation.
Healthcare providers may initially misdiagnose LS as recurrent candidiasis, contact dermatitis, psoriasis, vulvodynia, balanitis, or chronic eczema.
Since early lesions can appear subtle, diagnosis is frequently delayed until significant fibrosis has already developed.
Unfortunately, every year of persistent inflammation increases the likelihood of irreversible tissue remodeling.
Why Does Lichen Sclerosus Develop?
Despite decades of research, no single cause has been identified.
Instead, modern medicine considers LS a multifactorial immune-mediated disease resulting from complex interactions between genetic, environmental, immunological, and molecular factors.
Several mechanisms appear to contribute simultaneously.
Autoimmune Dysregulation
Perhaps the strongest evidence supports an autoimmune component.
Numerous studies demonstrate increased prevalence of autoimmune diseases among patients with lichen sclerosus, including:
- autoimmune thyroiditis;
- vitiligo;
- alopecia areata;
- type 1 diabetes mellitus;
- pernicious anemia;
- rheumatoid arthritis;
- systemic lupus erythematosus.
Patients frequently exhibit circulating autoantibodies directed against extracellular matrix protein 1 (ECM-1), suggesting abnormal immune recognition of structural proteins responsible for maintaining dermal integrity.
Activated T lymphocytes infiltrate affected tissue and produce numerous inflammatory mediators, including:
- interferon-γ;
- TNF-α;
- IL-1β;
- IL-6;
- IL-17;
- transforming growth factor-beta (TGF-β).
Persistent cytokine production maintains chronic inflammation even when external triggers have disappeared. New methods of autoimmune disease treatment: Autoimmune diseases and Stem cells therapy
 Chronic Inflammation
Chronic Inflammation
 Chronic Inflammation
Chronic InflammationUnlike acute inflammation, which promotes healing, chronic inflammation fundamentally alters tissue biology.
Continuous inflammatory signaling leads to:
- endothelial dysfunction;
- oxidative stress;
- mitochondrial injury;
- fibroblast activation;
- excessive collagen synthesis;
- extracellular matrix remodeling;
- vascular rarefaction.
Instead of repairing damaged tissue, inflammation begins driving fibrosis.
Over time, the tissue loses its capacity for physiological regeneration.
Fibrosis: The Central Driver of Disease Progression
Modern research increasingly identifies fibrosis—not inflammation alone—as the primary determinant of long-term disease progression.
Fibrosis develops when fibroblasts become chronically activated.
Under continuous stimulation by TGF-β and other profibrotic cytokines, fibroblasts differentiate into myofibroblasts, specialized contractile cells responsible for producing massive quantities of collagen.
Normal collagen turnover becomes disrupted.
Collagen type I gradually replaces the more flexible collagen type III.
Elastic fibers disappear.
Microvascular density declines.
The extracellular matrix becomes progressively rigid.
As a consequence:
- tissue contracts;
- elasticity is lost;
- blood supply decreases;
- epithelial regeneration slows dramatically;
- pain receptors become sensitized;
- chronic fissures develop.
This fibrotic transformation explains why even complete suppression of inflammation cannot always reverse advanced disease.
CONTACT
FOR FREE
CONSULTATION

Why Conventional Treatment Often Fails
For more than three decades, ultra-potent topical corticosteroids have remained the gold standard for the treatment of lichen sclerosus. Numerous clinical studies have demonstrated that these medications effectively reduce inflammation, relieve itching, decrease pain, and slow disease progression in a significant proportion of patients.
Despite their proven efficacy, corticosteroids do not eliminate the underlying biological mechanisms responsible for disease development. Instead, they primarily suppress the inflammatory response without restoring the damaged tissue architecture.
This distinction is critically important.
Many patients experience excellent symptom control during treatment, only to develop recurrent disease weeks or months after therapy is discontinued. Others gradually become less responsive to corticosteroids despite strict adherence to treatment recommendations.
The explanation lies within the biology of chronic tissue remodeling.
Once fibrosis has become established, simply suppressing inflammation cannot fully reverse the structural damage already present within the dermis and extracellular matrix.
Corticosteroids Control Inflammation—but Not Regeneration
The therapeutic activity of corticosteroids focuses primarily on reducing inflammatory cytokine production.
These drugs decrease the expression of:
- TNF-α
- IL-1β
- IL-6
- IFN-γ
- COX-2
- multiple inflammatory mediators
Consequently:
- itching decreases;
- erythema resolves;
- immune infiltration is reduced;
- tissue edema improves.
However, corticosteroids have only limited influence on several key biological processes responsible for long-term tissue degeneration.
These include:
- restoration of damaged collagen architecture;
- regeneration of elastic fibers;
- angiogenesis;
- stem cell niche recovery;
- extracellular matrix remodeling;
- mitochondrial dysfunction;
- epithelial stem cell activation.
As a result, inflammation may improve while fibrosis continues progressing at a microscopic level.
Progressive Fibrosis Continues Even During Clinical Remission
One of the most fascinating discoveries in modern fibrosis research is that chronic fibrotic remodeling may continue despite apparent clinical improvement.
 Patients frequently report:
Patients frequently report:
“My itching has disappeared, but the skin continues becoming tighter.”
“My symptoms improved, but the anatomy continues changing.”
“I no longer have pain, yet the tissue still feels rigid.”
These observations reflect ongoing extracellular matrix remodeling rather than active inflammation alone.
Fibrosis behaves almost like an independent biological program.
Activated myofibroblasts continue producing excessive collagen even after inflammatory cytokines decrease.
The extracellular matrix gradually becomes denser.
Elastic fibers remain fragmented.
Normal vascular architecture fails to recover.
Consequently, tissue mechanics continue deteriorating.
The Importance of Tissue Microenvironment
Healthy tissue regeneration depends on a highly organized biological ecosystem known as the tissue microenvironment.
This environment includes:
- resident stem cells;
- endothelial cells;
- fibroblasts;
- immune cells;
- extracellular matrix proteins;
- cytokines;
- growth factors;
- extracellular vesicles;
- neural signaling;
- vascular supply.
All of these components constantly communicate through highly sophisticated molecular signaling networks.
In lichen sclerosus this communication becomes profoundly disrupted.
Instead of regenerative signaling, tissues become dominated by inflammatory and fibrotic pathways.
As this imbalance persists, normal healing mechanisms gradually fail.
Stem Cell Exhaustion
Recent investigations suggest that chronic inflammation may progressively exhaust resident tissue stem cells.
Adult tissues continuously rely on small populations of progenitor cells responsible for replacing damaged epithelial cells and maintaining normal tissue homeostasis.
Persistent inflammatory cytokines impair this regenerative capacity.
Stem cell proliferation decreases.
Cellular senescence accelerates.
DNA damage accumulates.
Mitochondrial function deteriorates.
Consequently, tissue renewal becomes increasingly ineffective.
This phenomenon partly explains why advanced lichen sclerosus often demonstrates poor spontaneous healing.
Vascular Dysfunction
Healthy tissues require adequate oxygen delivery.
Chronic inflammation damages microvascular networks.
Capillary density decreases.
Endothelial dysfunction develops.
Local hypoxia increases.
Reduced oxygen delivery further stimulates fibrotic pathways through activation of hypoxia-inducible factor (HIF-1α).
Thus a vicious biological cycle emerges:
Inflammation →
vascular damage →
hypoxia →
fibrosis →
further inflammation.
Breaking this cycle represents one of the major goals of regenerative medicine.
Oxidative Stress
Another important contributor to disease progression is oxidative stress.
Inflamed tissues continuously generate:
- reactive oxygen species (ROS);
- free radicals;
- lipid peroxidation products.
Normally, antioxidant defense systems neutralize these molecules.
However, prolonged inflammation overwhelms endogenous antioxidant capacity.
Oxidative stress damages:
- mitochondrial DNA;
- nuclear DNA;
- cell membranes;
- proteins;
- extracellular matrix components.
The resulting molecular injury further accelerates fibrosis.
Mitochondrial Dysfunction
Mitochondria are no longer viewed simply as cellular power plants.
Modern cell biology recognizes mitochondria as central regulators of:
- energy production;
- apoptosis;
- immune signaling;
- inflammation;
- tissue regeneration.
Chronic inflammatory diseases frequently demonstrate impaired mitochondrial function.
Damaged mitochondria produce less ATP while generating greater quantities of reactive oxygen species.
This metabolic imbalance further impairs tissue repair.
Recent experimental studies suggest that restoration of mitochondrial function may improve cellular recovery in several chronic inflammatory diseases.
This concept has stimulated growing scientific interest in mitochondrial biology within regenerative medicine.
Why Regenerative Medicine Is Receiving Increasing Attention
Unlike conventional therapies that focus primarily on suppressing inflammation, regenerative medicine seeks to restore the biological environment required for normal tissue repair.
Rather than targeting a single cytokine or inflammatory pathway, regenerative therapies attempt to influence multiple interconnected biological systems simultaneously.
These include:
- immune regulation;
- angiogenesis;
- extracellular matrix remodeling;
- fibroblast behavior;
- stem cell activation;
- mitochondrial metabolism;
- intercellular communication.
This systems biology approach represents one of the defining characteristics of modern regenerative medicine.
Importantly, many regenerative strategies remain investigational for lichen sclerosus. While early laboratory and preliminary clinical findings are encouraging, robust randomized controlled trials are still needed before these approaches can be considered established standards of care.
Mesenchymal Stem Cells: Biological Conductors of Tissue Regeneration
Among all cell populations investigated in regenerative medicine, mesenchymal stem cells (MSCs) have become the most extensively studied.
Originally researchers believed MSCs repaired tissues by directly replacing damaged cells.
This concept has changed dramatically.
Current evidence indicates that the principal therapeutic activity of MSCs derives from their remarkable ability to orchestrate tissue repair through paracrine signaling.
In other words, MSCs function less as replacement cells and more as biological coordinators.
They communicate with surrounding cells by releasing hundreds of bioactive molecules.
These include:
- cytokines;
- chemokines;
- growth factors;
- extracellular vesicles;
- exosomes;
- regulatory microRNAs;
- anti-inflammatory proteins.
Together these molecules create an environment favorable for tissue regeneration.
Instead of forcing regeneration, MSCs encourage the body’s own repair mechanisms to resume normal function.
How MSCs May Influence Lichen Sclerosus
Experimental studies suggest several biological mechanisms through which mesenchymal stem cells may influence chronic inflammatory disorders.
These include:
Immune modulation
MSCs may reduce excessive activation of T lymphocytes while promoting regulatory immune responses.
Anti-inflammatory activity
They secrete IL-10, TGF-β modulators, prostaglandin E2, IDO, and numerous immunoregulatory molecules.
Anti-fibrotic effects
Experimental models suggest MSC-derived signaling may reduce myofibroblast activation and modulate collagen remodeling.
Angiogenesis
MSC secretome contains:
- VEGF
- HGF
- FGF
- angiopoietins
These molecules promote formation of new microvessels.
Extracellular matrix remodeling
Rather than simply degrading collagen, MSCs appear capable of regulating matrix metalloproteinases (MMPs) and tissue inhibitors (TIMPs), contributing to balanced remodeling of connective tissue.
Epithelial regeneration
Experimental evidence indicates MSC-derived growth factors may support proliferation of epithelial progenitor cells, improving tissue renewal.

 Mitochondrial Therapy and Cellular Bioenergetics
Mitochondrial Therapy and Cellular Bioenergetics Intravenous immunoglobulins (IVIG) are purified preparations of human antibodies that have long been used in selected immunodeficiency and autoimmune disorders. Beyond passive antibody replacement, immunoglobulins possess complex immunomodulatory properties, including regulation of Fc receptors, modulation of complement activation, neutralization of autoantibodies, and influence on cytokine production. In carefully selected patients with documented immune abnormalities, these effects may theoretically contribute to improved immune regulation. Nevertheless, IVIG is not a standard treatment for lichen sclerosus, and its use in this context remains investigational.
Intravenous immunoglobulins (IVIG) are purified preparations of human antibodies that have long been used in selected immunodeficiency and autoimmune disorders. Beyond passive antibody replacement, immunoglobulins possess complex immunomodulatory properties, including regulation of Fc receptors, modulation of complement activation, neutralization of autoantibodies, and influence on cytokine production. In carefully selected patients with documented immune abnormalities, these effects may theoretically contribute to improved immune regulation. Nevertheless, IVIG is not a standard treatment for lichen sclerosus, and its use in this context remains investigational.Lichen sclerosus is far more than a chronic inflammatory skin disorder. It is increasingly recognized as a complex immune-mediated disease characterized by persistent inflammation, progressive fibrosis, extracellular matrix remodeling, vascular dysfunction, oxidative stress, and impaired regenerative capacity. These interconnected biological mechanisms explain why many patients continue to experience disease progression despite receiving the current standard of care.
Although ultra-potent topical corticosteroids remain the cornerstone of conventional treatment and are highly effective in controlling symptoms and reducing inflammation, they do not directly restore damaged tissue architecture or reverse established fibrosis. This therapeutic limitation has driven growing scientific interest in regenerative medicine as a complementary strategy aimed at promoting tissue repair rather than symptom suppression alone.
During the past decade, advances in stem cell biology have fundamentally changed our understanding of tissue regeneration. Mesenchymal stem cells (MSCs), adipose-derived stem cells (ADSCs), Muse cells, extracellular vesicles, exosomes, secretome therapy, mitochondrial support, and immune modulation have emerged as promising investigational technologies capable of influencing multiple biological pathways simultaneously. Rather than acting through a single pharmacological mechanism, these regenerative products interact with immune cells, fibroblasts, endothelial cells, epithelial progenitors, and the extracellular matrix to help restore tissue homeostasis.
The concept of combination regenerative therapy is based on the understanding that chronic inflammatory diseases rarely result from a single pathological mechanism. Instead, they develop through a complex interaction of immune dysregulation, persistent cytokine activation, impaired angiogenesis, oxidative stress, extracellular matrix remodeling, and stem cell niche dysfunction. Consequently, future regenerative strategies are increasingly focused on restoring the biological microenvironment rather than targeting only one inflammatory pathway.
The investigational protocol described in this article reflects this systems biology approach by integrating cellular therapy with cell-free biological products and individualized immune support. While preliminary experimental and early clinical data are encouraging, it is essential to recognize that these therapies are still under active scientific investigation. Large, well-designed randomized clinical trials remain necessary to determine their long-term safety, optimal treatment protocols, patient selection criteria, and clinical efficacy.
The future of lichen sclerosus management will likely move beyond symptom control toward biological tissue restoration. As regenerative medicine continues to evolve, the integration of stem cell science, extracellular vesicle biology, molecular immunology, tissue engineering, and precision medicine may redefine the therapeutic landscape for patients living with chronic inflammatory and fibrotic diseases.
Ultimately, the goal of regenerative medicine is not simply to treat disease—but to restore the biological integrity, function, and regenerative capacity of human tissues. Find out the information how NK cells kill virus: NK cells help to kill herpes virus!
 Frequently Asked Questions (FAQ)
Frequently Asked Questions (FAQ)
 Frequently Asked Questions (FAQ)
Frequently Asked Questions (FAQ)1. What is lichen sclerosus?
Lichen sclerosus is a chronic inflammatory skin disorder that primarily affects the genital and perianal regions. It is characterized by progressive inflammation, tissue thinning, fibrosis, and architectural changes.
2. Is lichen sclerosus an autoimmune disease?
Although the exact cause remains unknown, substantial evidence suggests that autoimmune mechanisms play an important role in many patients.
3. What are the most common symptoms of lichen sclerosus?
Common symptoms include severe itching, burning, pain, skin whitening, fissures, discomfort during intercourse, and progressive scarring.
4. Can lichen sclerosus be cured?
Currently, there is no definitive cure. Most treatments aim to control inflammation, relieve symptoms, and reduce disease progression.
5. Why do corticosteroids sometimes stop working?
Corticosteroids effectively suppress inflammation but do not directly reverse fibrosis or restore damaged tissue architecture.
6. What causes fibrosis in lichen sclerosus?
Persistent inflammation activates fibroblasts, leading to excessive collagen production and progressive connective tissue remodeling.
7. What are mesenchymal stem cells (MSCs)?
MSCs are adult stem cells known for their immunomodulatory and regenerative properties. They primarily exert their effects through the release of bioactive signaling molecules.
8. Why are adipose-derived stem cells (ADSCs) used in regenerative medicine?
ADSCs are abundant, easily obtained, and produce a rich secretome containing growth factors, cytokines, and extracellular vesicles.
9. What are Muse cells?
Muse cells are a specialized population of endogenous reparative stem cells that may migrate to damaged tissues and participate in tissue regeneration.
10. What are exosomes?
Exosomes are nanosized extracellular vesicles that transfer proteins, RNA, microRNA, and signaling molecules between cells.
11. What is secretome therapy?
Secretome therapy uses the complete spectrum of bioactive molecules naturally secreted by regenerative cells to influence tissue repair.
12. Why are growth factors important?
Growth factors regulate angiogenesis, collagen remodeling, epithelial regeneration, and cellular communication.
13. What is mitochondrial therapy?
Mitochondrial-based regenerative strategies aim to improve cellular energy production and reduce oxidative stress.
14. Why is angiogenesis important in lichen sclerosus?
Healthy blood vessels provide oxygen and nutrients necessary for tissue regeneration and wound healing.
15. Can stem cells reduce fibrosis?
Experimental studies suggest that stem cell-derived signaling may help modulate fibrosis, although further clinical research is required.
16. Are exosomes a replacement for stem cells?
Not necessarily. Exosomes are being investigated as a complementary or cell-free regenerative approach.
17. Why is chronic inflammation difficult to eliminate?
Persistent immune activation continuously stimulates tissue remodeling and fibrosis, creating a self-perpetuating disease cycle.
18. Is combination regenerative therapy a standard treatment?
No. Combination regenerative therapy remains investigational and has not been established as a standard clinical treatment for lichen sclerosus.
19. Can regenerative medicine replace conventional therapy?
At present, regenerative medicine should be considered an emerging research field rather than a replacement for evidence-based standard treatments.
20. Why is personalized regenerative medicine becoming important?
Every patient demonstrates unique inflammatory, immunological, and regenerative characteristics. Personalized biological therapies aim to address these individual differences.
21. What role do cytokines play in lichen sclerosus?
Cytokines regulate immune activity, inflammation, fibrosis, and tissue repair. Abnormal cytokine signaling contributes to disease progression.
22. Can regenerative medicine improve tissue quality?
Current research suggests that regenerative approaches may support tissue remodeling and restoration of biological homeostasis, but further clinical evidence is needed.
23. Are stem cell therapies approved worldwide for lichen sclerosus?
No. Their use varies by country and regulatory framework, and most applications remain investigational.
24. What is the future of regenerative medicine for lichen sclerosus?
Future therapies are expected to combine stem cells, exosomes, secretome, biomaterials, molecular medicine, and precision immunology to create personalized regenerative treatment strategies.