
Treatment of COPD with Stem Cells and Bioactive Bioproducts: Potential, Mechanisms, and Clinical Observations
Chronic obstructive pulmonary disease (COPD) remains one of the leading causes of disability in older adults. Traditional treatment methods—bronchodilators, inhaled steroids, oxygen therapy, pulmonary rehabilitation—help reduce symptoms and slow disease progression, but they do not restore damaged lung tissue. This is why interest in regenerative technologies—stem cell therapy and the use of bioactive bioproducts (exosomes, growth factors, conditioned media)—has been growing in recent years.
Why Stem Cells Attract Attention in COPD
The main idea of cellular therapy is to influence not only the symptoms but also the underlying pathological processes. In COPD, the following occur:
• chronic airway inflammation
• destruction of alveolar septa
• loss of lung tissue elasticity
• impaired microcirculation
• reduced local immunity
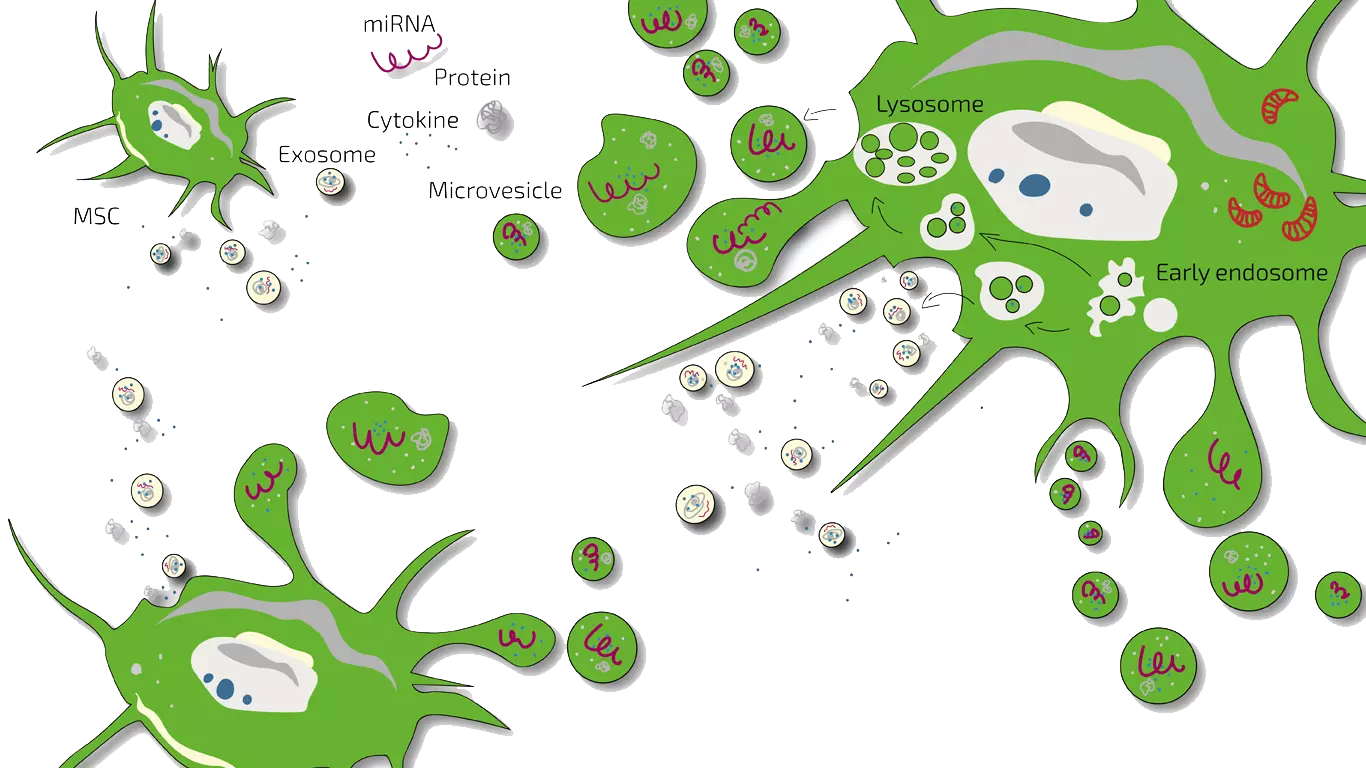
Mesenchymal stem cells (MSCs), used in most studies, are capable of secreting hundreds of regulatory molecules—cytokines, growth factors, peptides. They modulate immune function, reduce inflammation, improve microcirculation, and stimulate epithelial repair processes.

How the Therapy Affects Processes in the Lungs
Modern research shows that MSCs act primarily through paracrine signaling—by releasing biologically active substances. Key effects include:
• Anti-inflammatory effect
MSCs reduce pro-inflammatory cytokines (TNF-α, IL-6) and increase anti-inflammatory mediators. This helps reduce airway swelling and irritation.
• Anti-fibrotic action
Some bioproducts may slow down excessive connective tissue formation, important in emphysematous changes.
• Stimulation of angiogenesis and microcirculation
Improved blood supply enhances oxygenation and restores local immune function.
• Regeneration of the epithelial layer
Exosomes and growth factors support alveolar cell renewal and partially improve gas exchange.
• Immunomodulation
Bioproducts help reduce exacerbation frequency by normalizing immune activity.
It is important to understand that the goal is not complete lung regeneration but support of biological processes that can improve breathing function and quality of life.
More about stem cells therapy: How do stem cells work in the body?
Clinical Observations and Statistical Data
Since cellular technologies for COPD remain experimental, available statistics are based mainly on several clinical studies. In various studies conducted in recent years, the following were reported:
• improved exercise tolerance (greater 6-minute walk test distance)
• reduced dyspnea severity (mMRC, CAT scales)
• decreased exacerbation frequency during 12 months of follow-up
• improved FEV1 in some study participants
Bioactive Bioproducts: Exosomes and Conditioned Media
Exosomes are microscopic extracellular vesicles containing proteins, microRNA, and growth factors. They deliver “instructions” to lung tissue cells, regulating inflammation and regeneration.
Advantages of bioproducts:
• no risk of uncontrolled cell proliferation
• high concentration of active molecules
• ability to penetrate hard-to-reach lung regions
• potentially more predictable safety profile
Studies show that exosomes can reduce inflammation and support epithelial repair as effectively as MSCs themselves.
Biochemical Mechanisms of Improvement in COPD
Reduction of Chronic Inflammation (Immunomodulation)
COPD pathology is largely driven by persistent inflammation of lung tissue.
MSCs reduce inflammatory activity.
Key biochemical changes:
• ↓ TNF-α — main pro-inflammatory cytokine damaging lung tissue
• ↓ IL-1β, IL-6 — mediators maintaining chronic inflammation
• ↑ IL-10 — anti-inflammatory cytokine
• ↓ NF-κB activation — a master transcription factor of inflammation
Result: reduced swelling, less alveolar damage, and decreased extracellular matrix destruction.
Antioxidant Effect
COPD lungs experience constant oxidative stress.
MSCs:
• ↑ expression of SOD (superoxide dismutase)
• ↑ catalase
• ↑ glutathione peroxidase
Thus:
• reduced free radical levels
• less DNA and membrane damage
• slower epithelial cell death
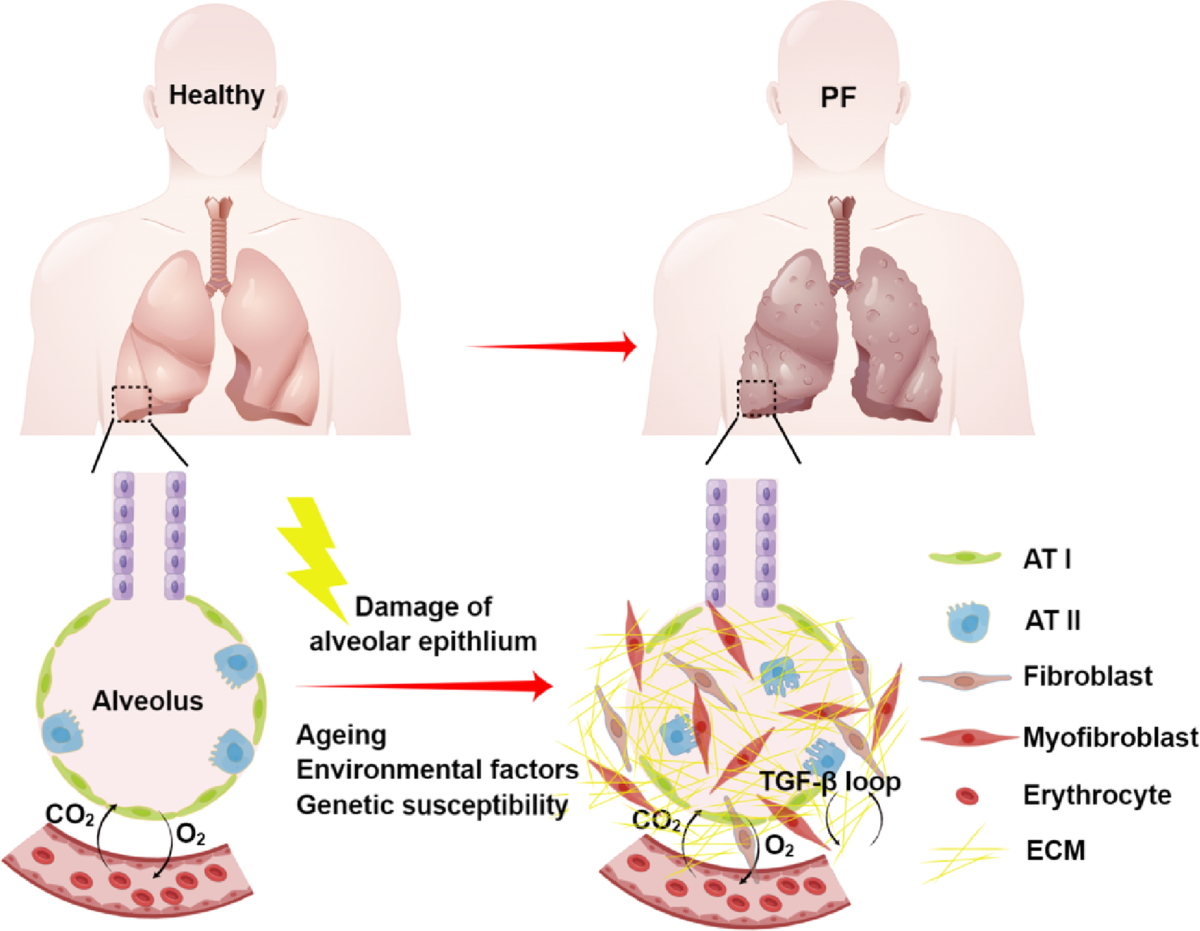
Remodeling and Restoration of the Extracellular Matrix
In COPD, the following are damaged:
• elastin
• collagen fibers
• alveolar wall structure
MSCs secrete:
• low-concentration TGF-β (high levels cause fibrosis; low levels support repair)
• FGF-2
• VEGF
• HGF
These molecules:
• stimulate synthesis of normal collagen and elastin
• enhance alveolar epithelial repair
• reduce tissue destruction by enzymes (e.g., metalloproteinases)
Result: more stable alveolar structure and slower emphysema progression.
Anti-apoptotic Action
Increased alveolar cell death is a major factor in COPD lung injury.
MSCs release factors that:
• ↓ caspase-3 expression
• ↑ Bcl-2 (anti-apoptotic protein)
This helps:
• preserve alveolar cells
• reduce alveolar wall thinning
• slow lung tissue destruction
Improved Microcirculation and Angiogenesis
COPD disrupts lung blood supply.
Endothelial stem cells secrete:
• VEGF
• PDGF
• ANG-1
Effects:
• capillary growth in damaged regions
• improved oxygen delivery
• reduced tissue hypoxia
• vascular endothelium restoration
Reduction of Fibrosis
Fibrosis (excess connective tissue formation) worsens lung function.
MSCs:
• ↓ excessive TGF-β
• ↓ fibroblast activity
• ↓ pathological collagen type I and III synthesis
This helps slow the formation of stiff, non-functional tissue.
Paracrine Regulation and Exosomes
Most MSC effects are due not to engraftment but to:
• release of exosomes containing proteins, RNAs, and anti-inflammatory molecules
• remote regulation of lung cell behavior
Exosomes:
• reduce inflammation
• support epithelial regeneration
• stabilize the alveolar barrier
This is currently one of the most active research directions.
What Happens to Lung Tissue
In the alveoli:
• reduced inflammation
• decreased septal destruction
• reduced alveolocyte death
• improved epithelial repair
• slower alveolar expansion and thinning (emphysema)
In the bronchi:
• reduced mucosal inflammation
• decreased mucus hypersecretion (via MUC5AC modulation)
• reduced wall edema
• improved small airway patency
In the pulmonary vasculature:
• improved microcirculation
• decreased pulmonary hypertension
Key Clinical Studies
-
Weiss et al., Chest 2013 — randomized, placebo-controlled study (N≈62)
— Design: systemic infusion of allogeneic MSCs (Prochymal) in moderate–severe COPD
— Result: safety confirmed; no significant improvements in FEV1 or QoL; early CRP reduction in patients with elevated baseline CRP -
Phase studies (allogeneic MSCs, UC-MSCs, ADSCs)
— Numerous small studies (typically dozens of patients)
— Report good safety, some improvements in quality-of-life measures (CAT, SGRQ) and 6MWT
— Mixed results for FEV1 and gas exchange
Clinical trial registries:
— Multiple ongoing protocols, including NCT00683722 (Prochymal)
What meta-analyses say
• Calzetta et al., 2022 (systematic review + meta-analysis)
— Trend toward FEV1 improvement (~+90 ml or more)
— Significant improvement in 6MWT (tens of meters; one analysis ≈+250 m)
— More stable reduction in exacerbation-related hospitalizations
Use of Specific Biobank-Derived Products in COPD Treatment
MITOCHONDRIA
Mitochondria play a key role in COPD because they determine cellular energy levels, inflammation, and oxidative stress. In COPD, mitochondria are damaged: they produce excess free radicals, generate insufficient ATP, activate inflammatory cascades, and induce alveolar cell apoptosis. When their condition improves, patient health improves.
Mitochondrial restoration reduces oxidative stress: fewer radicals are produced, antioxidant enzymes increase, lung damage slows. Cellular energy metabolism improves—ATP production increases; epithelium becomes more resilient; surfactant-producing cells and ion transport normalize, improving ventilation and gas exchange. Chronic inflammation decreases via reduced NLRP3 inflammasome and NF-κB activation, lowering IL-1β, TNF-α, and IL-6.
Normalization reduces apoptosis: less cytochrome c release, lower caspase activity, higher Bcl-2. This slows alveolar wall destruction. Respiratory muscle performance improves, especially the diaphragm—greater mitochondrial density, better oxidative phosphorylation, less fatigue, and improved exercise tolerance.
Mitophagy recovery removes damaged mitochondria, reducing intracellular inflammation and improving epithelial regeneration. Activation of PGC-1α, AMPK, and SIRT3 promotes biogenesis of new mitochondria.
Clinically this manifests as reduced dyspnea, improved oxygen saturation, better endurance, reduced chronic inflammation, and slower tissue destruction.
Macrophage Extracellular Vesicles (M2 Type)
M2 macrophages have strong anti-inflammatory activity.
M2 vesicles can:
• reduce neutrophilic inflammation
• lower IL-8 and neutrophil elastase
• protect tissue from destruction
• stimulate regenerative processes
This may be useful in the “neutrophil-dominant” COPD phenotype.
Cell-Free Conditioned Medium
Conditioned medium contains everything released by cells:
exosomes, cytokines, growth factors, lipids, metabolites.
Different cell-secretomes have shown:
• reduced inflammation
• accelerated tissue repair
• decreased fibrosis
• improved microvascular function
Advantage: absence of cellular components reduces risks.
Peptide Bioregulators and Matrix Extracts
Non-cellular biomaterials capable of modulating regeneration:
• extracellular matrix fragments
• purified matrix peptides
• microfibrous protein complexes
They can:
• reduce metalloproteinase activity
• decrease elastin destruction
• stimulate alveolar structure repair
Such products are used in regenerative technologies.
Exosomes of Immunoregulatory Cells
Vesicles from:
• regulatory T cells (Treg-EVs)
• myeloid-derived suppressor cells (MDSC-EVs)
They can:
• strongly suppress inflammation
• reduce the autoimmune component of COPD
• lower exacerbation frequency

Patient Feedback
Anna, 62, moderate COPD:
“After the course of bioproducts, I noticed less shortness of breath when climbing stairs. Dyspnea didn’t disappear but became more manageable. No exacerbations in six months.”
Wisam, 58, lung emphysema:
“I participated in a stem cell study. After a few months, I felt less fatigue and sleepiness. My lung function barely changed, but overall well-being improved.”
Lauren, 66, severe COPD:
“No miraculous cure, but my cough softened and breathing became a bit easier. The doctor said results vary. I’m satisfied because my quality of life improved.”
Mark, 67, Canada:
“I received mesenchymal cells. After a couple of months, climbing stairs became easier—I no longer needed frequent stops. Dyspnea remained but was milder. I walked farther in the 10-minute walk test. The doctor noted reduced inflammatory markers.”
Juan, 59, Spain:
“No immediate improvement after cell therapy, but after 3–4 months, exertion became easier, and nighttime coughing episodes decreased. I can’t say my lungs ‘recovered,’ but I have more energy.”
Elizabeth, 72, UK:
“I have severe COPD. After stem cell therapy, the first weeks were unchanged, but later I felt greater endurance while walking. Spirometry didn’t change much, but my condition stabilized with fewer exacerbations.”
Peter, 64, Germany:
“I joined a cell therapy study. Improvements were moderate—slightly easier breathing during exertion and fewer morning wheezes. The doctor reported reduced inflammatory markers. Even small changes felt important.”
Sarah, 51, USA:
“The biggest improvement was reduced fatigue—physical activity became less exhausting. I can walk longer now and had almost no exacerbations this year. Lung function improved slightly, but I feel the overall effect.”
These examples reflect a general trend: improvement is possible, but the degree varies depending on COPD stage, comorbidities, and individual physiology.
GET FREE ONLINE CONSULTATION

anti-inflammatory lung therapy, bioactive bioproducts COPD, chronic obstructive pulmonary disease stem cells, clinical trials stem cell COPD, COPD regenerative medicine, COPD treatment research, lung repair stem cells, mesenchymal stem cells COPD, MSC exosomes, stem cell therapy for COPD, stem cells for lung diseases, stem cells treatment for copd