
Very often, surgical interventions are accompanied by complications in patients. And even when surgery is performed with high quality, a patient may experience prolonged pain, discomfort, loss of sensitivity, long-lasting malaise, and other symptoms. Disorders may affect different areas of soft tissue, organs, or entire systems. After surgery, a process of injury and repair is initiated in the body, and disturbances can occur at various levels. Let’s break this down step by step.
Disorders in tissues and organs after surgery
-
Inflammatory changes
-
local edema, leukocyte infiltration;
-
excessive production of inflammatory mediators (cytokines, prostaglandins).
-
-
Necrosis/ischemia
-
when blood vessels are damaged or tissues are overstretched, some cells die → necrotic area.
-
-
Fibrosis and scarring
-
replacement of normal tissue with connective tissue (for example, a skin scar, adhesions in the abdominal cavity).
-
-
Adhesion formation
-
when serous membranes (peritoneum, pleura) are injured, adhesions develop → organ dysfunction.
-
-
Nerve damage
-
injury to nerve fibers can cause paresthesia, reduced motility (e.g., after limb or gastrointestinal surgery).
-
-
Infectious complications
-
wound infection, abscesses, systemic septicemia.
-
-
Organ dysfunction
-
resection leads to loss of functional tissue (e.g., nephrectomy, lung resection).
-
How tissue regeneration is disrupted
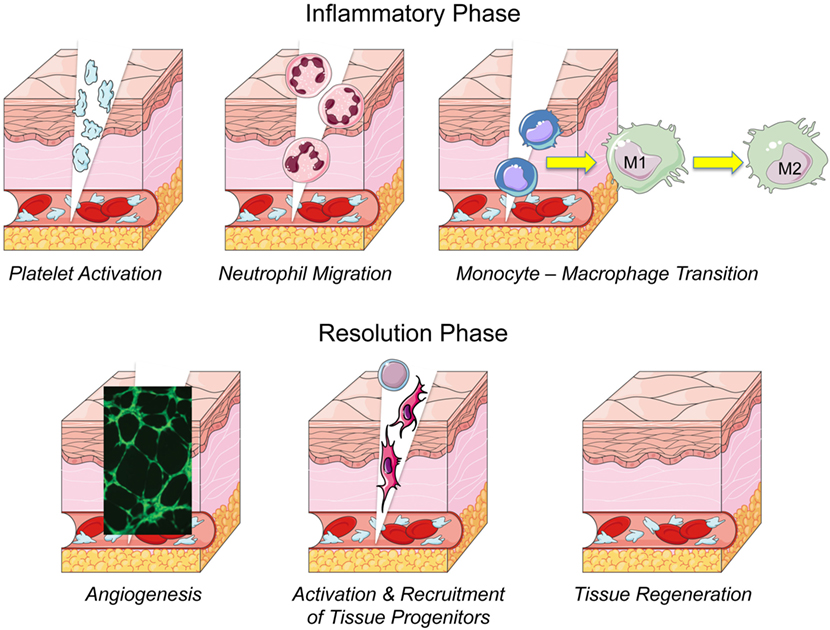
Normally, regeneration proceeds in 3 phases:
-
Inflammation (wound cleaning, immune cell migration).
-
Proliferation (growth of fibroblasts, endothelial cells, granulation tissue formation).
-
Remodeling (collagen maturation, tissue restoration).
Disruptions may occur at each stage:
-
Excessive inflammation → chronic healing, formation of coarse scar tissue.
-
Insufficient cellular proliferation (for example, in immunodeficiency, diabetes) → slow healing, chronic ulcers.
-
Impaired angiogenesis → tissue hypoxia, slowed repair.
-
Excessive fibrosis → keloid scars, contractures.
-
Impaired epithelialization → wound dehiscence, fistula formation.
Why this happens
-
Local factors
-
insufficient blood supply (ischemia, thrombosis);
-
wound infection;
-
mechanical tension or pressure on tissues;
-
necrosis due to trauma.
-
-
Systemic factors
-
diabetes mellitus → microvascular disorders + weak immune response;
-
vitamin deficiencies (C, A, zinc) → impaired collagen synthesis;
-
immunodeficiency (HIV, cytostatics, glucocorticoids) → weak proliferation;
-
advanced age → low regenerative potential;
-
smoking, hypoxia, anemia → poor oxygen delivery.
-
-
Surgical factors
-
prolonged surgery, massive tissue damage;
-
use of rough suture materials;
-
poor hemostasis or excessive coagulation → necrosis of wound edges.
-
In summary, after surgery, various organs and systems may experience inflammation, fibrosis, scarring, adhesions, necrosis, and infection. Regeneration is impaired due to a combination of local damage (ischemia, infection) and systemic factors (immunity, metabolism, age).

The role of stem cells in restoring regeneration
Stem cells of different types help repair damaged organs and tissues through several complementary mechanisms — directly replacing lost cells, creating a favorable environment for endogenous regeneration, and modifying the local immune and extracellular matrix landscape.
Some types, such as embryonic stem cells and induced pluripotent stem cells (iPSCs), have broad differentiation potential and theoretically can serve as a source of almost any specialized cells (cardiomyocytes, neurons, hepatocytes, etc.), making them highly attractive for replacing large volumes of lost parenchyma. With proper directed differentiation and purification, such cells can integrate into damaged tissue and functionally restore lost activities — for example, replacing dead cardiomyocytes after myocardial infarction or supplementing neuronal populations in neurodegenerative diseases.
Mesenchymal stromal/stem cells (MSCs) usually work not through massive differentiation but through strong paracrine and immunomodulatory effects. MSCs secrete a whole “secretome” of growth factors (VEGF, HGF, IGF, etc.), cytokines, and extracellular vesicles (exosomes) that stimulate angiogenesis, attract and proliferate endogenous tissue stem cells, reduce apoptosis in progenitor cells, and remodel the extracellular matrix. Moreover, MSCs can shift macrophages from the pro-inflammatory M1 phenotype to the reparative M2, suppress excessive T-cell activation through factors such as PGE2 and IDO, and thereby reduce chronic inflammation that interferes with regeneration. In practice, this translates into reduced fibrosis in liver and heart tissue, accelerated wound healing, and improved microcirculation in the damaged area. However, transplanted MSCs often show low survival and short lifespan; their therapeutic effect is largely realized in the first days to weeks through their secreted mediators.
Hematopoietic stem cells (HSCs) have historically been used to restore hematopoiesis and the immune system. In cases of massive loss or genetic defects, they can achieve long-term repopulation of the bone marrow and restore all blood cell lineages. Today, HSCs are also used as a platform for gene therapy: editing a patient’s own HSCs makes it possible to correct hereditary blood diseases and then return the engineered cells for permanent treatment. In this case, the mechanism is direct cell replacement and restoration of the normal function of the hematopoietic system.
Tissue-specific (resident) stem and progenitor cells — such as satellite cells in skeletal muscle, epidermal stem cells, neuronal progenitors, or hepatic precursors — play a central role in physiological regeneration. Therapeutic approaches can focus on stimulating them at the site of injury (via growth factors, small molecules, or modified secretomes) or expanding them ex vivo with subsequent transplantation. These cells integrate better into the tissue niche and carry a lower risk of immune rejection, but their numbers and reparative potential in adults are often limited, especially under chronic inflammation or age-related niche degeneration. Therapy, therefore, aims either to restore the niche or to support it with external cellular resources.
Vascular/endothelial progenitors and other pro-angiogenic cells are critical for restoring blood supply to damaged areas; without adequate neovascularization, transplanted cells and repaired parenchyma quickly die from hypoxia. Thus, successful regenerative strategies often combine cells that stimulate vessel formation with growth factors or biomaterials that support angiogenesis and provide oxygen and nutrients during the early stages of engraftment.
In addition, the field of “cell-free” therapy is rapidly developing: the use of extracellular vesicles (exosomes) rich in proteins, microRNAs, and lipids that reproduce many of the therapeutic effects of cells (anti-apoptotic, pro-angiogenic, immunomodulatory) with significantly fewer risks compared to living cells.

Bioengineering approaches and biomaterials significantly enhance the potential of cell therapy. Delivering cells within hydrogels, scaffolds, or 3D-bioprinted constructs with controlled mechanics and porosity increases their survival, directs differentiation, and accelerates integration with host tissue. Genetic modification of cells (for example, to increase stress resistance, boost the production of specific growth factors, or eliminate oncogenic risks) adds another level of control and allows adaptation to specific pathologies. Combined approaches — cells plus scaffold plus molecular “support” — offer the best chances for stable regeneration.
Ultimately, different types of stem cells provide different tools for repair: some allow direct replacement of specialized cells, others deliver strong paracrine and immunomodulatory support, and others serve as the foundation for tissue engineering and vascular restoration. In practice, effective strategies usually combine several approaches — cellular material, bioactive factors, and appropriate biomaterial scaffolding — and require individualized design for a specific organ, type of damage, and patient condition.
Therefore, when selecting biobank products, we always focus on the specific case of the patient, the current tissue or organ damage, the symptoms caused by this damage, and the assessment of how particular biomaterials may adapt and function in that case.
complications after surgery how to help, Endothelial regeneration treatment with stem cells, exosomes for regeneration, extracellular vesicles in tissue regeneration, iPSC Therapy Effects in tissue regeneration, liver regeneration therapy, nerve regeneration, recovery after surgery, Regeneration of cardiomyocytes, regeneration power of stem cells, Stem cells for stimulation testicular tissue regeneration, stem cells in tissue regeneration, Tissue regeneration after surgery with stem cells, Tissue regeneration with stem cells, Tissue-specific (resident) stem and progenitor cells in tissue regeneration, to cure damages after surgery, to regenerate hepatocytes, Vascular/endothelial progenitors in tissue regeneration