
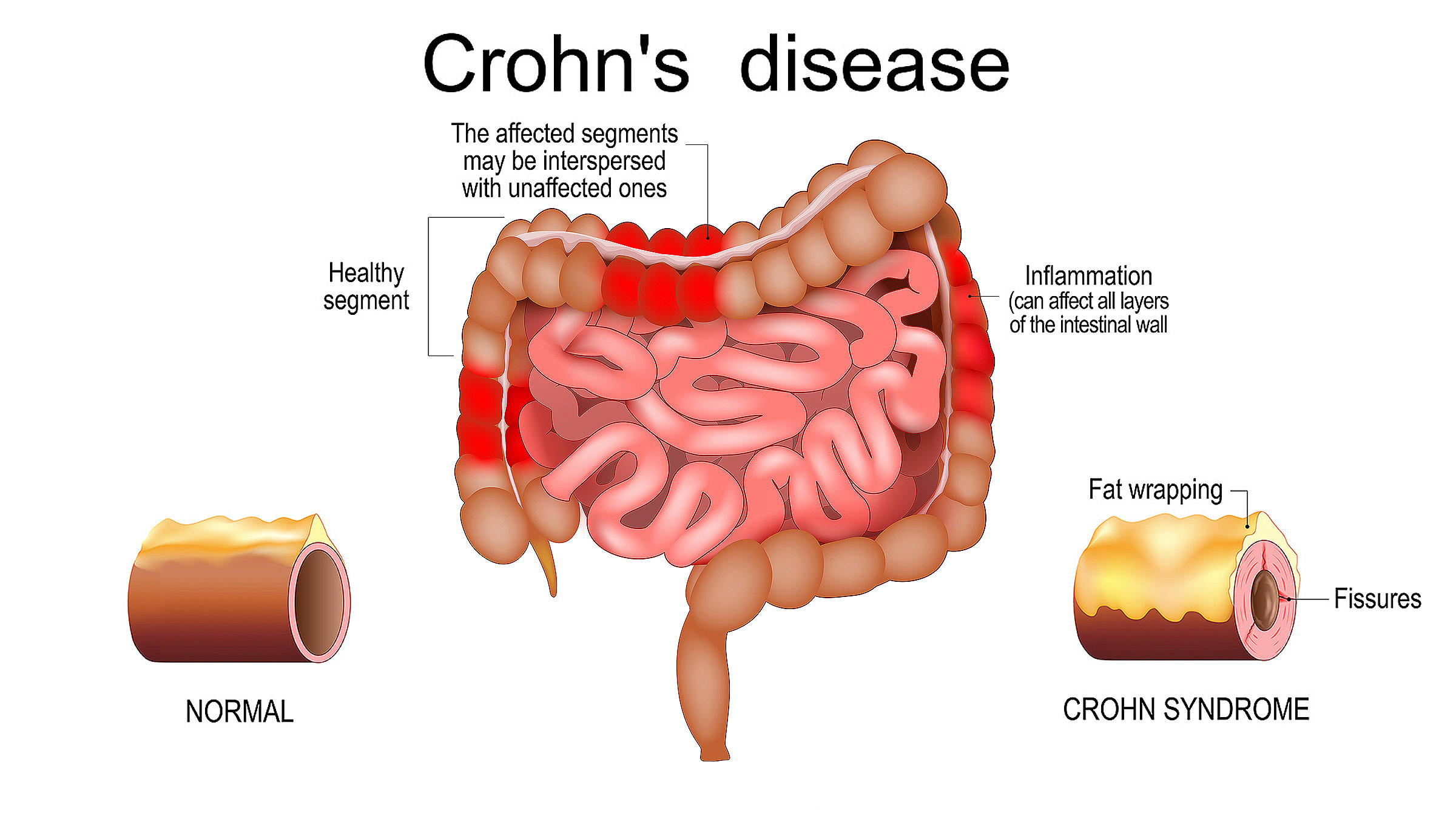
Crohn’s Disease is a chronic inflammatory bowel disease (IBD) that can affect any part of the gastrointestinal tract, from the oral cavity to the anal canal. Its nature is multifactorial: genetic predisposition, immune system dysfunction, microbiota imbalance, and environmental factors.
Nature and Pathogenesis of Crohn’s Disease
1. Genetic predisposition
More than 200 genes have been identified as associated with increased risk, including NOD2/CARD15, ATG16L1, IL23R.
These genes are linked to bacterial recognition, autophagy (cellular clearance of damaged structures), and regulation of inflammatory responses.
Carriers of these mutations have an immune system that responds abnormally to components of normal gut microbiota.
2. Immunological disturbances
Normally, the immune system distinguishes between “self” (own tissues and beneficial bacteria) and “non-self” (pathogens).
In Crohn’s disease, this balance is disrupted → gut microbiota is perceived as a threat
This triggers chronic inflammation, characterized by:
hyperactivation of Th1- and Th17-lymphocytes,
increased production of cytokines (TNF-α, IL-6, IL-12, IL-23),
reduced regulatory mechanisms (deficiency of Treg cells that normally suppress inflammation).
3. Role of microbiota
Patients often exhibit dysbiosis: a decrease in beneficial bacteria (e.g., Faecalibacterium prausnitzii) and overgrowth of conditionally pathogenic bacteria (adhesive E. coli).
This enhances immune stimulation, perpetuating the “vicious cycle” of inflammation.
4. Environmental factors
Smoking increases risk 2–3 times.
A diet high in fat and sugar, and low in fiber worsens the course of the disease.
Stress, infections, and antibiotic use can trigger exacerbations.
Stepwise Changes in Crohn’s Disease
1. Initiation
In a predisposed individual, the intestinal epithelium comes into contact with altered microbiota.
Defective barrier mechanisms (mucus, tight junctions) allow bacterial components to penetrate deeper.
2. Activation of innate immunity
Macrophages and dendritic cells become activated and release proinflammatory cytokines (TNF-α, IL-1β).
Neutrophils are recruited, causing mucosal damage.
3. Activation of adaptive immunity
T-helper cells (Th1, Th17) are activated, producing IFN-γ, IL-17, IL-22.
A chronic inflammatory focus is established, maintained by continuous microbiota stimulation.
4. Chronic inflammation and tissue damage
Prolonged immune response leads to granulomas (clusters of macrophages and lymphocytes).
Intestinal wall thickening, strictures (narrowing), and fistulas develop.
Vascular damage and ongoing inflammation cause bleeding, anemia, and malabsorption.
Crohn’s disease is an autoimmune-like condition in which the immune system loses the ability to adequately recognize normal microbiota and begins to attack its own intestines. Genetic predisposition, dysbiosis, and hyperactivation of inflammatory pathways (Th1/Th17 → TNF-α, IL-23, IL-17) play key roles. Stepwise changes — from barrier dysfunction to chronic inflammation with granulomas — lead to severe clinical manifestations.
Application of iPSCs in Crohn’s Disease
Crohn’s disease is associated with immune dysfunction and disruption of the intestinal barrier.
iPSCs can generate immunoregulatory cells (e.g., mesenchymal stromal cells, Tregs) and intestinal epithelial cells/organoids to restore damaged mucosa.
Thus, therapy works in two directions:
-
-
Immunomodulation (reducing aggressive inflammatory response).
-
Regeneration of intestinal epithelium (restoring barrier and mucosal integrity).
-
iPSC Protocol for Crohn’s Disease
1. Harvesting and preparation of material
-
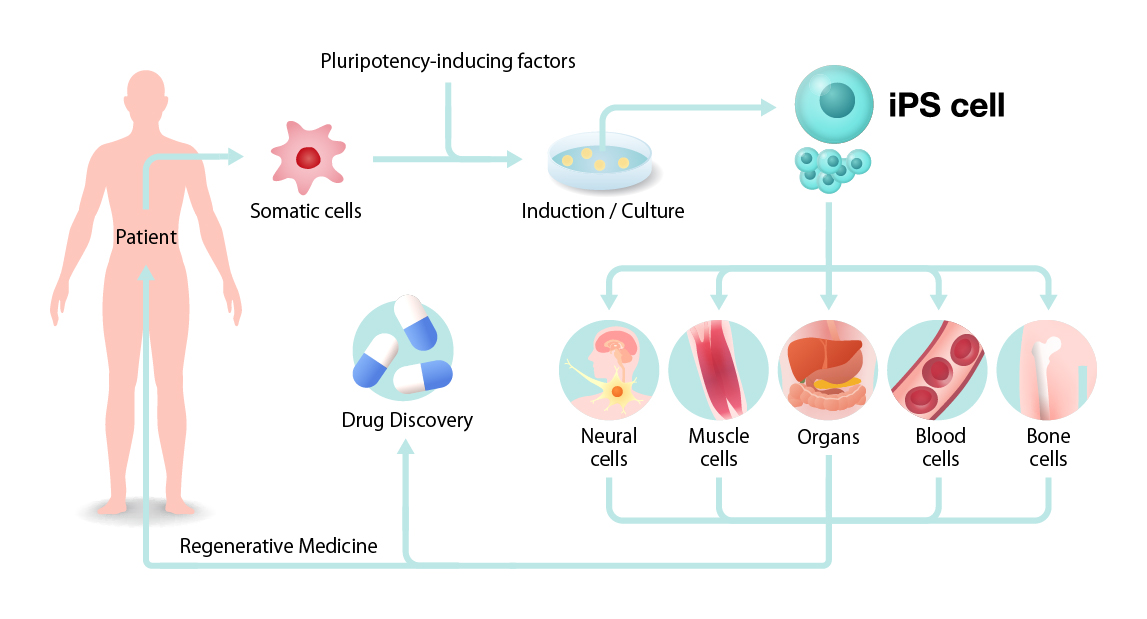
Obtain patient’s somatic cells (most often peripheral blood mononuclear cells).
-
Reprogram these cells into iPSCs using transcription factors (Oct4, Sox2, Klf4, c-Myc).
2. Cultivation and differentiation
-
Create two lines of cellular derivatives:
-
Immunomodulatory cells: iPSC → mesenchymal stromal cells (MSC) or regulatory T-cells (iPSC-Treg).
-
Intestinal epithelial cells: iPSC → enterocytes, goblet cells, epithelial organoids.
-
3. Quality control
-
Assess genetic stability (exclude mutations, tumorigenesis risk).
-
Test secretory profile (growth factors, anti-inflammatory cytokines IL-10, TGF-β).
-
Confirm absence of contamination and endotoxins.
4. Administration to patient
-
Intravenous infusion of iPSC-MSC: systemic anti-inflammatory effect (reduces TNF-α, IL-6, IL-17, activates Treg).
-
Endoscopic administration of epithelial organoids into affected gut areas: mucosal and barrier restoration.
-
Local administration of iPSC-MSC exosomes (intravenous or mucosal): stimulate regeneration, suppress inflammation without tumorigenic risk.
5. Supportive therapy
-
Diet supporting microbiota (prebiotics, probiotics, avoiding inflammatory triggers).
-
Correction of vitamin D, B12, iron deficiencies to enhance cell therapy efficacy.
6. Monitoring
-
Immunological control: cytokine levels (IL-6, TNF-α, IL-10), Th17/Treg balance.
-
Morphological control: endoscopy, mucosal biopsy.
-
Clinical dynamics: frequency of flare-ups, pain reduction, weight restoration.
Expected Effects
-
Immune modulation: reduced chronic inflammation, restored Treg control.
-
Mucosal regeneration: restored epithelial barrier, fewer ulcers and erosions.
-
Complication reduction: fewer strictures, fistulas, anemia.
-
Clinical improvement: fewer relapses, improved quality of life.
Using iPSCs in Crohn’s disease is a strategy combining immune modulation and mucosal regeneration. This protocol theoretically allows not only suppression of inflammation but also repair of damaged tissue. In practice, iPSC-derived MSCs and exosomes are used more frequently today, as they are safer.
Recent studies and clinical observations have shown encouraging results in the use of stem cell therapy for Crohn’s disease. Patients with this chronic and often debilitating inflammatory bowel condition have demonstrated significant improvements in both symptoms and overall quality of life after undergoing stem cell-based treatments. Stem cells appear to address two key pathological processes of the disease: excessive immune activation and structural damage to the intestinal mucosa. By exerting strong immunomodulatory effects, they reduce the overproduction of proinflammatory cytokines such as TNF-α and IL-6, while enhancing the activity of regulatory T-cells that help control inflammation. This leads to a decrease in flare frequency, reduced intestinal pain, and lower dependence on corticosteroids and immunosuppressants.
Beyond immune regulation, stem cells have shown the ability to support regeneration of the intestinal lining, promoting mucosal healing and restoration of the barrier function that is often severely compromised in Crohn’s patients. Clinical outcomes have included closure of fistulas, reduction in strictures, and improved absorption of nutrients, resulting in fewer complications such as anemia and weight loss. Importantly, patients treated with mesenchymal stem cells or induced pluripotent stem cell derivatives have often maintained remission for prolonged periods, sometimes for years, especially when combined with supportive therapies.
Overall, stem cell therapy offers a unique dual action—suppressing harmful immune responses while simultaneously stimulating tissue repair. These combined effects make it one of the most promising strategies for managing Crohn’s disease, not only in controlling inflammation but also in reversing some of the structural damage that conventional therapies cannot address. While large-scale randomized trials are still ongoing, the current evidence strongly suggests that stem cells can achieve results unattainable with standard treatments, giving hope for long-term remission and better quality of life for patients living with Crohn’s disease.

Duration of iPSC Therapy Effects in Crohn’s Disease
1. iPSC-MSC (mesenchymal cells from iPSC)
Survive only briefly after intravenous infusion.
Their paracrine effects (anti-inflammatory cytokines, exosomes) can maintain remission from several months to 3–5 years, depending on disease stage and inflammation intensity.
2. iPSC-derived intestinal epithelial organoids
If successfully integrated, can live and divide for years, restoring barrier function.
Strong inflammation or relapse may damage them.
Typically effective for 24 months or longer, especially with supportive therapy (diet, medication).
3. iPSC-Treg or immune cells
Their lifespan depends on immune microenvironment.
Under strong inflammation, Tregs may become depleted quickly.
Remission usually lasts 16 months to 3–5 years, provided inflammatory triggers are controlled.
4. iPSC/MSC exosomes
Circulate in blood for only days but trigger cascades of regeneration and immune correction.
Require repeat courses every 12–18 months to maintain effect.
Factors Determining Duration of Effect
-
Disease stage
Early stages (less structural damage): longer effect.
Advanced stages with strictures, fibrosis, fistulas: shorter effect.
-
Cell type and administration method
Local organoid transplantation → longer effect (can engraft).
Systemic MSC/iPSC-MSC infusion → faster onset, shorter duration.
-
Patient’s immune status
Strong autoimmune activity or persistent Th17 activation can shorten effect.
Immunosuppressive support prolongs action.
-
Microbiota
Uncorrected dysbiosis allows pathogenic bacteria to reignite inflammation.
-
Lifestyle and environmental factors
Smoking, stress, poor diet → shorten remission.
Healthy nutrition and vitamin support (D, B12, iron) → prolong effect.
Conclusion
Short-term effect (reduction of inflammation, symptom relief): within weeks.
Medium-term effect (remission): 6–12 months.
Long-term effect (mucosal regeneration, fewer relapses): usually after 10–12 months, lasting 3 years or longer, sometimes more with successful organoid integration.