
Vaccination against COVID-19 has played a key role in combating the pandemic, significantly reducing the number of severe cases and mortality. However, in practical medicine, frequent cases of adverse reactions are recorded, including autoimmune and cardiovascular complications.
Autoimmune reactions after vaccination
Several studies indicate a possible link between vaccination and the development of autoimmune diseases. A review article notes the appearance of glomerulonephritis, autoimmune rheumatic diseases, and hepatitis after vaccinations. Molecular mimicry, activation of “bystander” lymphocytes, and the adjuvant effect of vaccines are discussed as potential triggers.
A Mendelian randomization study found a statistical association between vaccination and an increased risk of multiple sclerosis, Parkinson’s disease (OR ≈ 1.5), and ulcerative colitis (OR ≈ 1.00). A Korean cohort study showed that mRNA vaccination increases the risk of more than a dozen autoimmune diseases, except for systemic lupus erythematosus (risk increase of ~16%).
Clinical observations include ANCA-type vasculitis, thyroid diseases (Graves’ disease and subacute thyroiditis), autoimmune hepatitis, and neurological disorders such as ADEM, Guillain–Barré syndrome, and others.
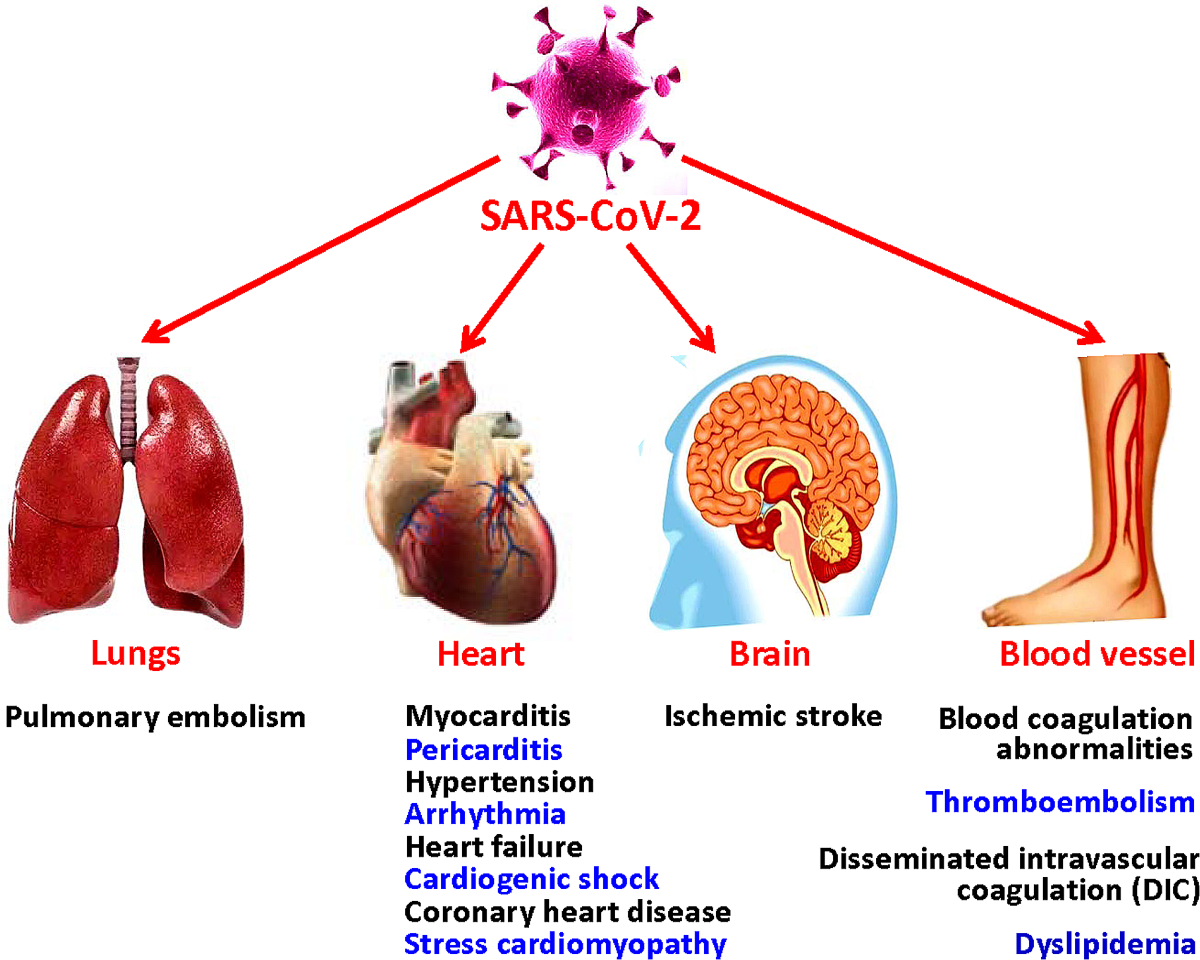
Cardiovascular complications
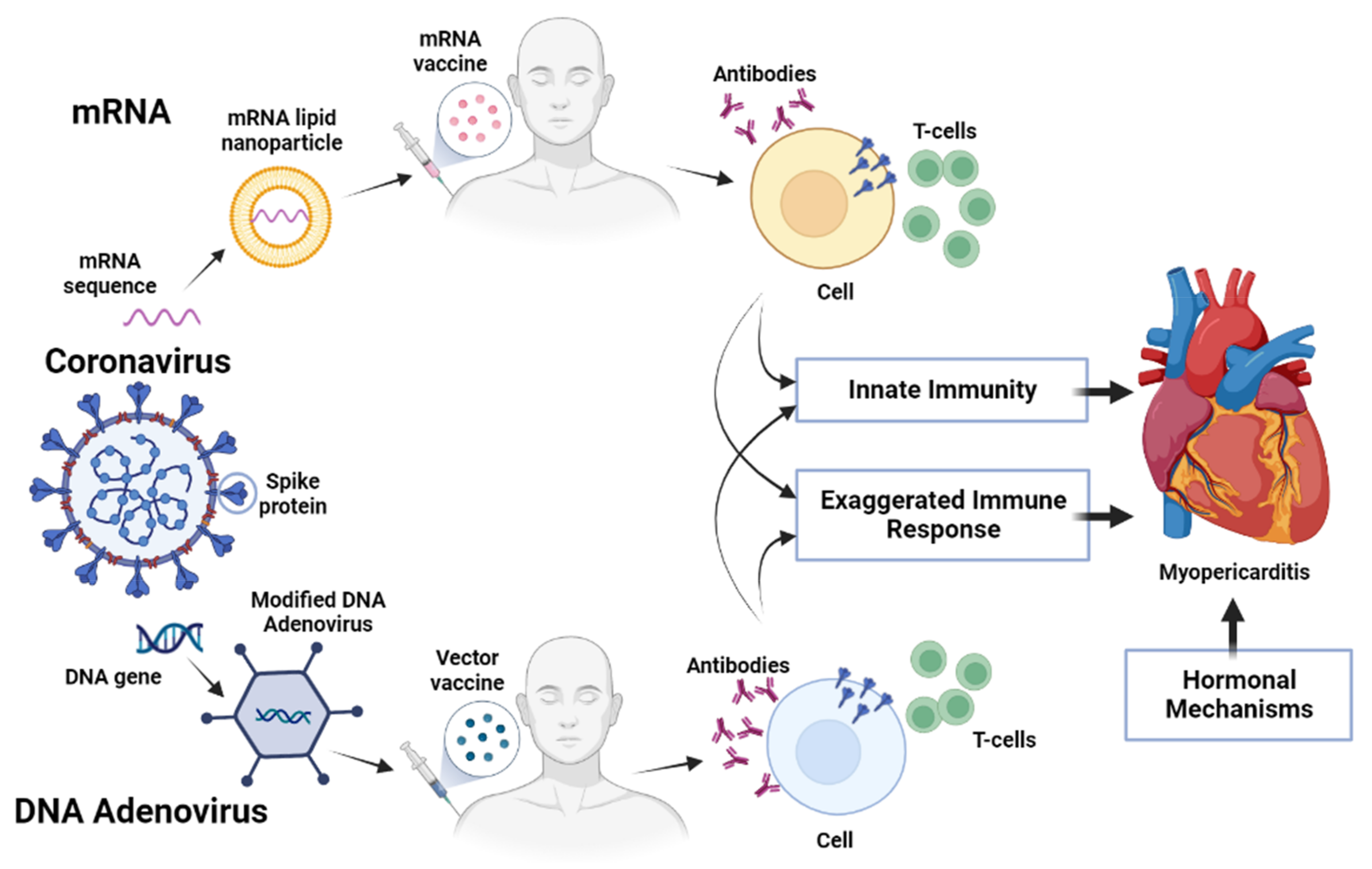
Cases of myocarditis in young men, most often after mRNA vaccines, deserve special attention. Thrombotic events (especially with adenovector vaccines) have also been reported.
Other complications
Some patients noted exacerbation of dermatological diseases such as psoriasis or eczema. In patients with lupus, mild reactivation is possible, although severe flares are extremely rare.
Why the immune system may aggravate autoimmune responses after vaccination
The human immune system after vaccination may exacerbate autoimmune responses due to the way it is activated and recognizes antigens. The mechanisms are complex, but several key processes are usually considered at the biological level:
- Molecular mimicry
Protein fragments (epitopes) of the SARS-CoV-2 virus introduced with the vaccine (e.g., in the form of mRNA or protein antigen) may structurally resemble the body’s own proteins. As a result, activated T and B lymphocytes may mistakenly attack tissues containing these “similar” proteins. - Epitope spreading
The vaccine stimulates a strong immune response, sometimes accompanied by tissue damage (even minimal). This releases additional antigens from cells previously hidden from the immune system, leading to an immune reaction not only to the viral antigen but also to self-proteins. - Bystander lymphocyte activation
During vaccination, the immune system releases a large number of cytokines and activates innate immunity. Sometimes this leads to the accidental activation of T cells that were already “on the verge” of autoimmune response but previously remained inactive. - Adjuvant effect
Some vaccines (especially non-mRNA) contain adjuvants—substances that enhance the immune response. In rare cases, strong stimulation of innate immunity can trigger autoimmune inflammation in predisposed individuals. - Genetic and epigenetic predisposition
People with certain HLA gene variants (e.g., HLA-B27, HLA-DR3, HLA-DR4) or with pre-existing immune tolerance disorders (subclinical forms of autoimmune diseases) have a higher risk that strong immune stimulation after vaccination will lead to exacerbations.
Risk of exacerbations in subclinical autoimmune diseases after vaccination
1. Exacerbations in patients with established autoimmune diseases
A systematic review showed an overall flare risk of about 16.3% after COVID-19 vaccination in patients with autoimmune-mediated diseases (AI-IMD).
According to the COVAD study, about 1 in 10 patients with autoimmune rheumatic diseases experienced exacerbations, ranging from 9.5% to 36.7%, depending on the method of assessment (self-reports, increased immunosuppression, etc.).
2. New autoimmune diseases after vaccination
A large US study found that the risk of developing a new autoimmune disease within one year after vaccination was about 28% compared to unvaccinated individuals. However, a significant increase was noted only for certain diagnoses: celiac disease (1.8×), autoimmune thyroiditis (1.7×), Sjögren’s syndrome (1.5×), and some others.

Why vaccination affected the older population more
In older patients, complications after COVID-19 vaccination were more common for several interconnected reasons, rooted in both the biology of aging and the characteristics of the immune system at this age.
- Immunosenescence — age-related decline in the number and function of T and B lymphocytes, changes in innate immunity, and increased production of pro-inflammatory cytokines. This results in a less balanced immune response: antibody production may be weaker, while inflammatory reactions can be stronger and longer-lasting.
- Multiple chronic diseases — cardiovascular, endocrine, autoimmune, pulmonary. These conditions increase the risk of adverse events after any major immune stimulation, including vaccination. This is especially true for those with decompensated heart disease, diabetes, chronic kidney failure, or pre-existing autoimmune disorders.
- Polypharmacy — simultaneous use of multiple medications. Some drugs (immunosuppressants, anticoagulants, corticosteroids) can alter the response to vaccines, increase the risk of side effects, or mask early signs of complications.
- Inflammaging — chronic low-grade inflammation in aging makes the body more vulnerable to additional inflammatory triggers like antigen exposure from vaccination. This can worsen tissue damage, autoimmune shifts, or chronic disease decompensation.
Comparative table: Young vs. Elderly immune response
| Component / Aspect | Young organism | Elderly organism |
|---|---|---|
| Innate immunity (neutrophils, macrophages, dendritic cells) | Rapid activation, efficient phagocytosis, and antigen presentation | Reduced phagocytosis, impaired antigen presentation, slower initial reaction |
| Adaptive immunity – T-cell response | Strong CD4+/CD8+ proliferation, good effector & memory T generation | Reduced naïve T cells, lower proliferation & function, shift to senescent T cells |
| Adaptive immunity – B-cell & antibody response | High antibody titers, good affinity, and class switching (IgG) | Lower antibody titers, slower affinity maturation, weaker class switching |
| Immune memory formation | Reliable long-term memory (B & T cells) | Less stable, shorter memory; needs boosters |
| Cytokine reactivity | Well-regulated, pronounced (reactogenicity) | May be blunted or dysfunctional (↑ inflammaging) |
| Inflammaging | Low/moderate | Moderately high; predisposes to stronger systemic reaction |
| Risk of acute complications | Low absolute risk; reactions (pain, fever) short-lived | Higher risk of chronic disease decompensation, thromboembolism, CV events |
| Impact of comorbidities & drugs | Fewer drugs → fewer interactions | Common comorbidities & polypharmacy ↑ risk of adverse effects |
| Need for adapted vaccination schedules | Standard doses & intervals | May require boosters, higher doses, adjuvanted vaccines, more monitoring |
| Recovery & disease reactivation | Quick recovery | Higher risk of chronic disease flare-ups (CV, metabolic, autoimmune) |
Stem cells and other bioproducts from biobanks for post-vaccination complications
Why this is relevant for people with post-vaccination complications
After vaccination, a small group of patients (especially elderly and those with chronic diseases) may develop:
- Hyperactive or dysregulated immune response → autoimmune processes, cytokine storm, vasculitis.
- Endothelial damage → thrombosis, microangiopathy.
- Chronic systemic inflammation → post-COVID-like fatigue syndrome, fibromyalgia-type pain.
- Organ damage (heart, nervous system, endocrine glands) due to autoimmune reactions or inflammation.

How stem cells may work
Stem cells have not so much a “replacing” effect as a regulatory one:
- Immunomodulation — MSCs reduce overactive T & B lymphocytes, increase regulatory T cells (Treg), balancing immune response.
- Anti-inflammatory action — suppress pro-inflammatory cytokines (IL-6, TNF-α) and shift towards anti-inflammatory (IL-10).
- Tissue regeneration — stimulate angiogenesis, activate local progenitor cells, repair damaged endothelium.
- Neuroprotection — release growth factors (BDNF, NGF) that protect and restore nerve tissue.
- Antifibrotic effect — reduce pathological organ scarring.
Other biobank products
- Exosomes & extracellular vesicles from MSCs — act as “biological nanoparticles” carrying anti-inflammatory and regenerative signals without introducing live cells (lower risk).
- Endothelial progenitor cells — restore vascular lining after vasculitis and microangiopathy.
- Allogeneic regulatory immune cells (Treg) — targeted suppression of autoimmune responses.
- Bioproducts enriched with growth factors — localized stimulation of tissue repair.
Why this may be especially useful for elderly patients
Their immune system is often locked in a state of chronic inflammation (inflammaging).
Stem cells can reduce this background “noise” and give tissues a chance to recover.
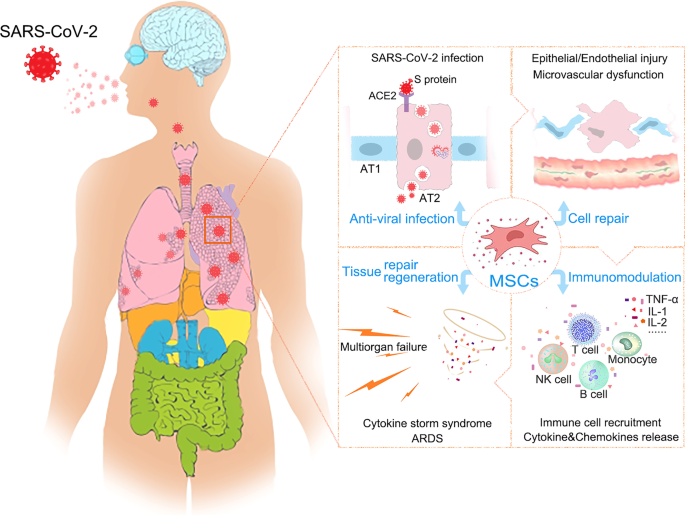
Table: Complication type – mechanisms – potential bioproducts – mechanism of benefit
| Type of complication | Possible mechanisms | Potential cells / bioproducts | Mechanism of benefit |
|---|---|---|---|
| Autoimmune reactions(e.g., rheumatoid arthritis, lupus flare) | Dysregulation of T & B lymphocytes, activation of autoreactive clones | MSCs, Treg cells | Suppress autoimmune response, stimulate regulatory T cells, reduce IL-6 & TNF-α |
| Vasculitis, endotheliopathy, microthrombosis | Endothelial damage, coagulation activation | Endothelial progenitor cells, MSC exosomes | Repair vascular lining, stimulate angiogenesis, suppress vascular inflammation |
| Neurological complications(polyneuropathy, neuritis, cognitive issues) | Neuroinflammation, myelin/axon damage | MSCs, neural progenitors, MSC exosomes, growth factors (BDNF, NGF) | Reduce neuroinflammation, remyelination, stimulate neuroregeneration |
| Myocarditis, pericarditis | Autoimmune or viral-like myocardial inflammation | Cardiac stem cells, MSCs | Anti-inflammatory effect, stimulate cardiomyocyte regeneration, improve microcirculation |
| Chronic fatigue syndrome, fibromyalgia | Low-grade systemic inflammation, mitochondrial dysfunction | MSCs, mitochondrial transplants, exosomes | Reduce inflammation, improve cellular energy metabolism |
| Endocrine complications(thyroiditis, type 1 diabetes) | Autoimmune attack on endocrine glands | MSCs, Treg, exosomes | Immunomodulation, protection & partial restoration of gland tissue |
| Chronic disease exacerbation | Systemic stress & inflammatory cascades | MSCs, PRP, growth factor-rich plasma | General anti-inflammatory support, stimulate damaged tissue regeneration |