
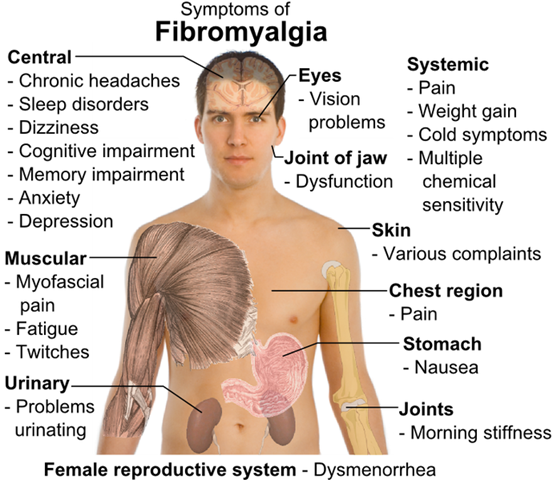
Fibromyalgia is a chronic pain syndrome characterized by diffuse pain in the muscles and soft tissues, fatigue, sleep disturbance, and cognitive dysfunction. Although the condition has only been officially recognized in recent decades, its mechanisms remain partly mysterious. However, research is bringing us closer to understanding its causes and risk factors.
Fibromyalgia is not a disease of the muscles, but a disorder of the central nervous system. Modern science views fibromyalgia as a dysfunction of central sensory pain processing—meaning that the brain and spinal cord process pain signals improperly, amplifying them even in the absence of external stimuli. This condition is called central sensitization. People with fibromyalgia experience pain more intensely due to hyperactivity in pain pathways and dysfunction in systems that suppress pain impulses.
Why fibromyalgia develops: a complex of causes
Genetic predisposition—studies show that 25–50% of patients have close relatives with similar symptoms. Genetic variants related to serotonin, dopamine, and catecholamine metabolism have been identified—neurotransmitters that play a critical role in pain perception and mood.
Trigger events—in many patients, fibromyalgia develops after a stressful event:
severe viral infection (including COVID-19), surgery, a car accident, childbirth, emotional or physical trauma.
These events can act as a “trigger,” especially in individuals with already heightened nervous system sensitivity.
Chronic stress and sleep disturbances—it has been demonstrated that prolonged sleep disruption (especially loss of deep sleep) amplifies pain sensitivity. Persistent stress and anxiety can also exhaust the central pain regulation system.
Hormonal and neurochemical imbalances—patients with fibromyalgia often exhibit low levels of serotonin, dopamine, and norepinephrine, along with elevated levels of substance P—a neuropeptide that intensifies pain signaling. Dysregulation of cortisol, the stress hormone, has also been found.
Who is most commonly affected: risk groups
Women comprise more than 80–90% of all cases. This may be linked to estrogen levels and hormonal cycles.
Age—most commonly arises between 30–50 years, though it can affect adolescents and the elderly.
Individuals with anxious, depressive, or obsessive traits
People with autoimmune diseases (e.g. lupus, rheumatoid arthritis)
Patients with a history of chronic pain syndromes (e.g. migraines, irritable bowel syndrome)
What increases the risk of developing fibromyalgia
Chronic insomnia
Psycho-emotional burnout
Sedentary lifestyle
Past injuries to the spine or head
Increased pain sensitivity since childhood
Family history of fibromyalgia
Frequent viral infections
Chronic deficiency of vitamin D, magnesium, B‑group vitamins

Fibromyalgia is not an “imaginary” illness
Fibromyalgia is a real neurological condition characterized by altered pain perception. It is not psychosomatic, but rather the result of a complex interaction between genetics, neurobiology, stress, and environment. Early diagnosis and comprehensive therapy—including medications, cognitive-behavioral therapy, physical exercise programs, and now regenerative medicine modalities (including stem cells)—significantly improve patient quality of life.
What changes occur in the body with a fibromyalgia diagnosis
Fibromyalgia is a complex, multifactorial disorder rooted in dysregulation of central and peripheral pain control, as well as biochemical dysfunction in neurotransmitter, hormonal, and immune systems. At a biological level, the key mechanism is central sensitization—the state in which the central nervous system becomes hypersensitive to painful and non-painful stimuli.
As a result, even normal touch, muscle tension, or light pressure are perceived as painful. This is driven by increased activity of neurons in the dorsal horn of the spinal cord and decreased function of descending inhibitory pathways that normally suppress pain.
Neurochemically, fibromyalgia is accompanied by deficiencies in neurotransmitters such as serotonin, dopamine, and norepinephrine. These substances regulate mood and emotional tone, and also modulate pain. Their deficit diminishes the activation of antinociceptive mechanisms, while substance P—a neuropeptide that amplifies pain transmission—is elevated in patients by nearly 2–3 times above normal.
Expanded activity of NMDA (glutamate) receptors also occurs, which amplifies pain transmission and fosters persistent neuronal activation. This combination disrupts the brain’s filtering of pain signals: any stimulus is perceived as stronger and more prolonged than it actually is.
Additionally, fibromyalgia disrupts the hypothalamic‑pituitary‑adrenal (HPA) axis. Reduced cortisol secretion, particularly in response to stress, can contribute to chronic inflammation and decreased ability to adapt to external challenges.
Despite the lack of classic tissue inflammation, there are signs of mild systemic inflammation—elevated levels of cytokines like IL‑6, IL‑8, and TNF‑α. This points to immune dysfunction involving microglia—brain immune cells that, when activated, release inflammatory mediators and sustain a state of hypersensitivity.
Functional alterations are also seen in specific brain regions associated with pain perception: increased activity in the thalamus, insular cortex, anterior cingulate cortex, and somatosensory cortex. These areas are involved not only in sensing pain but also in its emotional interpretation, which explains the commonly observed symptoms of anxiety, depression, cognitive disruption, and persistent fatigue.
Peripherally, even in the absence of overt inflammation or muscle damage, patients may exhibit impaired muscle metabolism—reduced local blood flow, hypoxia, and lactate accumulation—which contribute to sensations of pain and stiffness.
In summary, fibromyalgia represents a state in which pain regulation breaks down at all levels—from molecular and cellular processes to full neural networks in the brain—and is characterized by an imbalance between pro- and anti-nociceptive mechanisms, neuroinflammation, neurotransmitter deficiencies, and disruptions in hormonal and metabolic homeostasis.
Treatment of fibromyalgia with narrowly differentiated cells
In treating fibromyalgia, the primary interest is not the undifferentiated iPSCs themselves but their narrowly differentiated derivatives, aimed at restoring specific impaired functions of the central nervous system and correcting biochemical dysfunctions.
The fundamental pathology in fibromyalgia—central sensitization—is caused by an imbalance between excitatory and inhibitory neurotransmitters, neuroinflammation, and underactive antinociceptive pathways in the brain and spinal cord. Narrowly differentiated iPSC-derived cells allow targeting these abnormalities at the cellular and molecular level.
First, iPSCs can be differentiated into inhibitory interneurons (e.g. GABAergic neurons) that contribute to the suppression of pain impulses. Delivered into relevant regions of the spinal cord or brainstem, these cells could theoretically enhance natural pain inhibition, which is especially important in patients whose anti-pain pathways are underperforming.
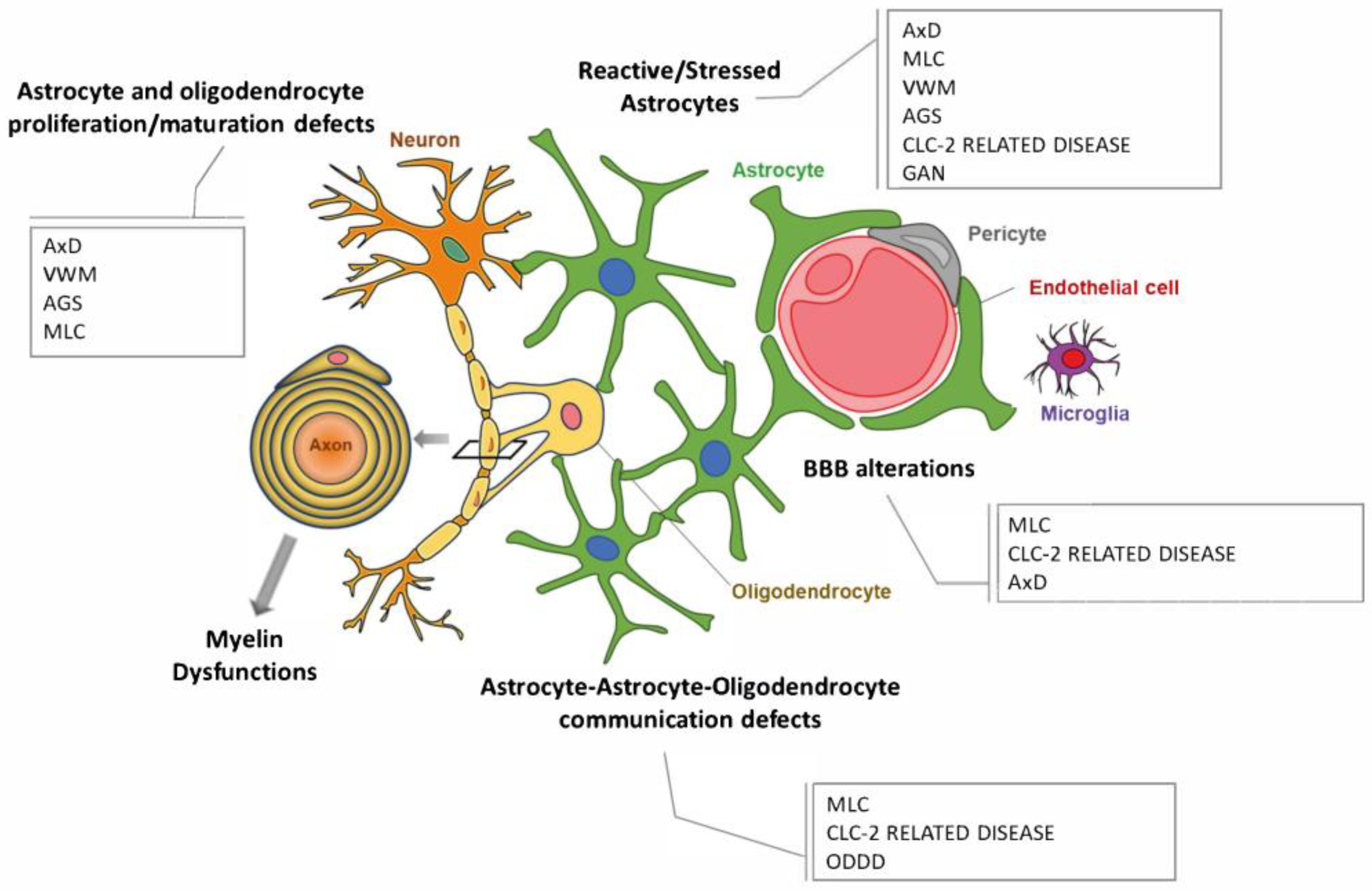
Second, iPSCs can be differentiated into astrocytes and oligodendrocytes capable of modulating inflammatory responses and maintaining CNS homeostasis. Astrocytes, in particular, regulate levels of glutamate, substance P and other mediators whose excess contributes to pain chronification. Modified astrocyte lines derived from iPSCs may be used to restore glutamate balance and reduce neuroinflammation.
A third direction is generating dopaminergic or serotonergic neurons, which participate in descending antinociceptive pathways. In fibromyalgia, levels of serotonin and dopamine are reduced, and restoring them may relieve pain symptoms, mitigate depression, and reduce fatigue.
Injections of such neurons (in future, with appropriate safety) could help normalize neurochemical balance.
Additionally, early-stage research explores personalized in vitro anti-pain neuroplatforms: iPSCs obtained from a fibromyalgia patient are differentiated into neurons, and various drugs are tested on them to individually tailor therapy, minimizing side effects and maximizing efficacy.
Thus, narrowly differentiated iPSC-derived cells—by restoring impaired inhibitory neural networks, reducing neuroinflammation, normalizing neurochemical balance and modulating pain sensitivity—have the potential to significantly alleviate fibromyalgia symptoms.
Clinical results in chronic neuropathic pain
In a pilot study involving ten patients with trigeminal neuralgia, autologous stromal vascular fraction (SVF) derived from adipose tissue was used. After six months, five of nine participants experienced a statistically significant reduction in pain (from 7.5 to 4.3 on the NRS scale, p = 0.018) and reduced doses of neuropathic pain medications.
• In a 2016 study (Stem Cells Translational Medicine, 36 patients), MSC therapy (adjuvanted MSCs from various sources) led to approximately 25% pain reduction and about 50% improvement in quality of life at six months compared to placebo.
• In 2018 (Stem Cell Reports, 20 patients), treatment with adipose-derived MSCs accompanied immune modulation, reduced inflammation, improved sleep and mood, and reduced central sensitization.
• In 2021, iPSC-derived neuronal products were used experimentally to restore neurotransmitters and reduce central sensitization, yielding positive preliminary outcomes.
• At Stanford in 2024, bioengineered MSCs with enhanced anti-inflammatory properties were used to modulate glial activity and restore autonomic regulation—significantly reducing fibromyalgia symptoms.
General outcome patterns
• Safety and tolerability: no serious adverse effects, complications, or immune reactions were reported in the studies.
• Impact on pain and quality of life: average pain reduction ranged from 20% to 55% within 3–6 months after infusion.
• Other clinical improvements: reductions in fatigue, normalization of sleep, and improvements in cognitive function and mood were reported.
• Underlying mechanisms: anti-inflammatory/immunomodulatory effects (reduction in IL‑6, TNF‑α, IL‑8), glial cell modulation, and restoration of neurotransmitter balance—linked to MSC and iPSC-derived therapy.
GET FREE ONLINE CONSULTATION
