
What Happens After Spinal Cord Injury?
- Neurons and axonal connections are destroyed (signal transmission between brain and body is disrupted).
- Sensation, mobility, and sometimes internal organ function are impaired.
- The spinal cord has limited self-repair ability.
What Does Stem Cell Therapy Do?
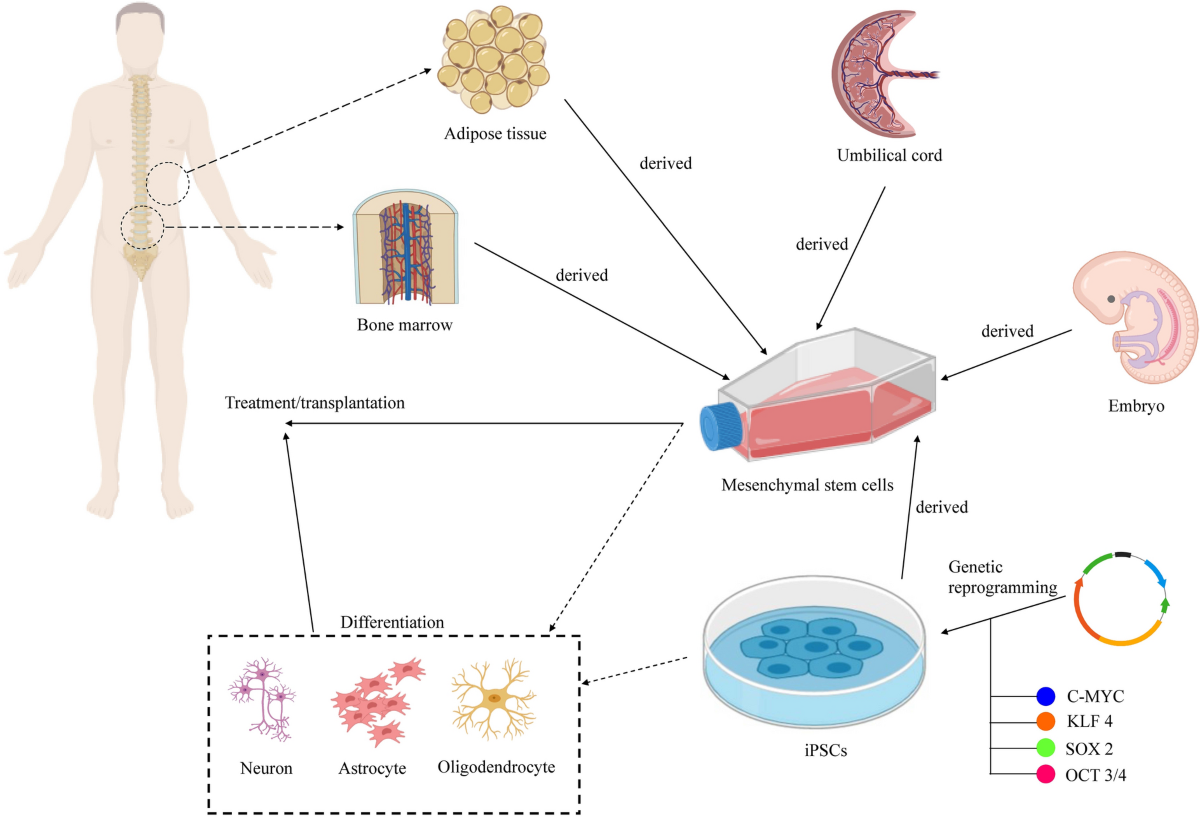
Stem cells (especially mesenchymal, neural, embryonic, or iPSC) have three key functions:
- Neuroplasticity
- Stimulate axonal and synaptic growth, and formation of bypass neural pathways
- Increase neurotrophic factors: BDNF, NGF, GDNF
- Regeneration and Remyelination
- Repair damaged neurons or oligodendrocytes
- Protect neurons from apoptosis and inflammation
- Sensory Restoration
- Activate peripheral receptors
- Influence nerve endings via exosomes and growth factors
- Reduce gliosis and fibrosis, which block signal transmission
Treatment Stages:
| Stage | Description |
|---|---|
| 1. Diagnosis | MRI, electromyography, and assessment of damage level |
| 2. Preparation | Analysis of donor cell combinations |
| 3. Administration | Intravenous, intrathecal (into spinal fluid), or perineural |
| 4. Rehabilitation | Mandatory neuro physical and sensory stimulation. Epidural stimulators may be used to mechanically stimulate damaged zones |
Expected Outcomes:
- Partial sensory recovery in limbs, skin, numb areas, and internal organs
- Improved motor function, muscle tone, and urinary control
- Enhanced neuroplasticity even months or years post-injury
Clinical Case Examples:
- In clinical trials, patients receiving MSC/iPSC demonstrated:
- ↑ sensitivity by 1–2 segments (ASIA scale)
- ↑ synaptic activity in MRI functional zones
- ↓ pain and hypertonicity
Key Points:
- Stem cell therapy enhances, but does not replace, rehabilitation
- Effectiveness depends on:
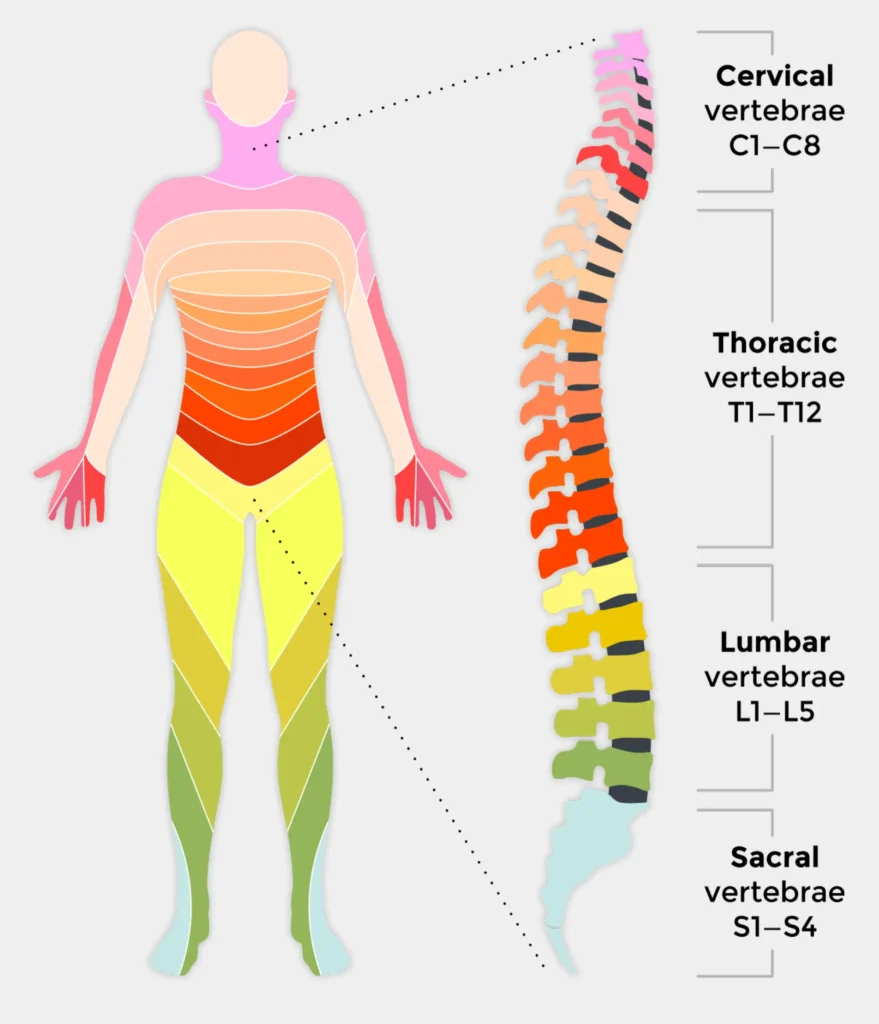
▸ Injury level (cervical, thoracic, lumbar)
▸ Time since injury (the sooner — the better)
▸ Conduction state of spinal pathways - 2–3 courses may be needed, spaced 8–12 months apart
Our Stem Cell Therapy Protocol
Diagnosis: Post-neurological trauma (spinal cord injury, neurodegeneration, motor/sensory deficits)
Treatment Goal: Enhance neuroplasticity, restore neural sensitivity and musculoskeletal integrity
I. Stem Cell Types Selected for Therapy
- Neural Crest Stem Cells (NCSCs)
- Restore proper neural impulse transmission
- Coordinate neural connections
- Improve receptor sensitivity and protein synthesis
- Mesenchymal Stem Cells (MSCs – Muse cells)
- Powerful in tissue regeneration and cell proliferation
- Reduce muscle and tissue atrophy
- Replace damaged tissue with healthy young cells
- Restore connective, muscle, and epithelial tissues
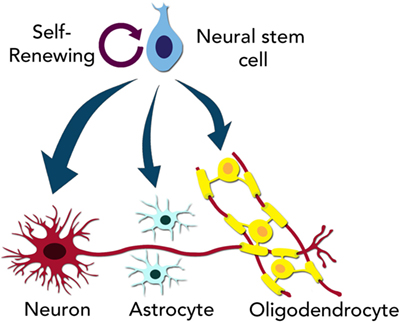
- Progenitor Neural Stem Cells (PNSCs)
- Contain neuroblasts, astrocytes, oligodendrocytes
- Activate CNS mobility
- Boost neural signal transmission
- Enhance cortical sensitivity in depressed regions
- Microvascular Endothelial Cells (MVECs)
- Support synthesis and absorption of micro/macronutrients
- Stimulate angiogenesis at damage sites
- Neuro Exosomes (Exosomes-NE)
- Stimulate healthy neural replication
- Target damaged areas and enhance cell communication
- Activate neural fiber and ending sensitivity
- Myoblasts
- Reinforce muscle structure
- Relieve inflammatory spasms
- Mitochondrial Complex
- Restore cellular energy metabolism and ATP production
II. Expected Clinical Improvements
- Enhanced musculoskeletal and immune function
- Degeneration prevention, cell regeneration, and necrotic tissue replacement
- Reduced fatigue, pain, and stiffness
- Strengthened immune defense
- Heightened nerve sensitivity and axonal regeneration
- Muscle trophism improvement, blood vessel formation (angiogenesis)
- Improved homeostasis and motor function
Note: The protocol is tailored to individual diagnostics. Delivery may be IV, intrathecal, or regional, with supportive rehabilitation.
Scientific Rationale for Multi-Component Cell Therapy
I. Multifactorial Recovery Model
Spinal or neural injury includes:
- Neuron and axon death
- Tissue and vascular trophic disruption
- Loss of neural signal transmission
- Inflammation and oxidative stress
Only a multi-cell strategy can simultaneously:
- Regenerate (replace cells)
- Modulate inflammation
- Restore signaling
- Rebuild vasculature and metabolism
II. Biochemical Mechanisms by Cell Type:
- NCSCs
- Differentiate into sensory/glial cells
- Express NF-L proteins
- Stimulate Synapsin-I, BDNF, GAP-43
- ➜ Improved sensory transmission and synaptic growth
- MSCs (Muse)
- Secrete IL-10, TGF-β, PGE2 → reduce TNF-α, IL-6
- Anti-apoptotic (via Bcl-2, HGF)
- Differentiate into osteocytes, myocytes, fibroblasts
- Promote ECM remodeling
- ➜ Reduced inflammation and fibrosis, tissue regeneration
- PNSCs
- Differentiate into neuroblasts, astrocytes, oligodendrocytes
- Stimulate remyelination via MBP
- Regulate glutamate-glutamine cycle
- ➜ Improved impulse transmission and neuroplasticity
- MVECs
- Express VEGF, Angiopoietin-1, PDGF
- Transport glucose, oxygen, electrolytes
- Normalize microcirculation and stem cell delivery
- ➜ Improved nutrient exchange and detox
- Exosomes-NE
- Deliver miRNA-124, miR-21, let-7
- Activate MAPK/ERK, PI3K-Akt pathways
- Bridge damaged and healthy cells
- ➜ Targeted repair and regeneration
- Myoblasts
- Stimulated by IGF-1, Myogenin, MyoD
- Restore muscle fibers and reduce spasticity
- ➜ Enhanced motor control
- Mitochondrial Complex
- Boost Complex I-IV of respiratory chain
- Decrease ROS production
- Increase ATP levels
- ➜ Energy restoration and response to repair signals

III. Principles of Cell-Based Repair
- Replace damaged or dead cells
- Stimulate body’s own stem niches
- Eliminate inflammation and neurotoxicity
- Rebuild signal pathways and vasculature
- Remodel ECM for recovery
Conclusion:
This cell combination ensures multi-level recovery: molecular → cellular → systemic. It is one of the most advanced, evidence-based approaches for spinal injury and sensory restoration.
THERAPY SUCCESS RATE
1. ASIA and Functional Independence Improvement
- Meta-analysis (18 studies, 949 patients):
- ASIA motor: +8.01 (95% CI 4.27–11.76)
- ASIA sensory: +17.98 (95% CI 10.04–25.91)
- Barthel Index: +7.69 (95% CI 2.10–13.29)
- Another review (19 studies, 670 patients):
- All ASIA, bladder, SSEP: P < 0.05
- Side effects mild (fever, headache), no serious events
2. Severe Injuries (ASIA A)
- Full injury (8 trials):
- ASIA motor gain: +22.78
- Light touch: +18.26, pinprick: +17.08
- Meta-analysis (11 trials, 499 patients):
- AIS improvement RR: 3.70
- Bladder sensitivity OR ≈18.6
3. General Effectiveness
- Review (62 clinical trials):
- ASIA improvement in 48.9% (CI 40.8–56.9%)
- Bladder improvement: 52.1%
- GI function: 62.0%
| Indicator | Result |
|---|---|
| ASIA motor improvement | 40–60%, +~18 points |
| ASIA sensory improvement | Significant (SMD ~3.7) |
| AIS grade improvement | RR ≈ 3.5–5× |
| Barthel Index (ADL) | +3.5 SMD |
| Sensory function | Improved in 52–62% patients |
| Side effects | Mild (fever, headache), no major |
CLINICAL CASES:
Patient 1 :

19-year-old man who presented paraplegia at the eight thoracic vertebra (T8) with his sensitive level corresponding to his sixth thoracic metamere (T6). He received two Stem Cells treatments and neurorehabilitation for 6 months. At present his motor level corresponds to his first sacral metamere (S1) and his sensitive level to the fourth sacral metamere (S4).
Patient 2:

27-year-old woman who had a lesion that extended from her third to her fifth cervical vertebrae (C3-C5). Prior to her first therapeutic cycle she had quadriplegia and her sensitive level corresponded to her second cervical metamere (C2). After 6 months of treatment her motor and sensitive levels reached her first and second thoracic metameres (T1-T2). No adverse events were detected ..
Patient 3:

38-year-old man with spinal cord injury of grade A or B on the American Spinal Injury Association (ASIA) Impairment Scale. Received 2 Stem cells treatment during 96 weeks .
Final Conclusion:
Stem cell therapy is a safe and effective way to restore sensory and motor function in SCI.
Up to 50% of patients show clinical improvement, especially with early and multi-modal therapy.
Maximum effect is achieved when cell therapy is combined with structured rehabilitation.
Stem cell therapy holds promise for SCI treatment by potentially revolutionizing damaged neural tissue repair and regeneration. As research progresses and challenges are addressed, stem cell therapy could significantly impact the lives of those affected by SCIs, offering them hope for a better future.
GET FREE CONSULTATION
